Form of Vitamin D: some need fatty meals, some respond quickly, etc.
Vitamin D Forms Comparison
†"Bioavailability" = intestinal absorption into lymph/portal circulation relative to maximum achievable — not serum 25(OH)D increase, which depends on additional metabolic steps.
| Form | Bioavail. without fat† | Bioavail. with fat† | Time to peak response | Acute-care suitability |
|---|---|---|---|---|
| Plain vitamin D D3 oil/powder capsule |
Low 1 | High 2 | 25(OH)D peaks ~7 days after single dose; full plateau after ~3 months of daily dosing 3 | Not suitable Weeks-scale response too slow for acute needs |
| Water-dispersible D3 Micellar / emulsified D3 |
Moderate 4 | High 4 | Similar curve to plain D3; fat-independence is the key advantage; same weeks-to-months timeline 5 | Limited Useful for fat malabsorption; still too slow for true acute care |
| Liposomal vitamin D Phospholipid vesicles |
High 6 | High 6 | Faster initial absorption vs. plain D3; 25(OH)D rise measurable within 1–3 days of loading; still weeks to full plateau 7 | Limited Best fat-independent oral option; days-scale, not hours |
| Calcifediol 25(OH)D — storage form (Rx in some countries) |
High 8 | High 8 | Serum 25(OH)D rises within 4–8 h of a loading dose; bypasses hepatic 25-hydroxylation step 9 | Good Hours-scale response; preferred oral agent for ICU loading (e.g. SCCM protocols, COVID-19 trials) 10 |
| Calcitriol 1,25(OH)₂D — active form (Rx) |
High 11 | High 11 | Biological effect within hours; peaks ~3–6 h post-dose; half-life only ~5–8 h — effects are short-lived 12 | Ideal — with caution Fastest VDR activation; IV form available; narrow therapeutic window — hypercalcemia risk 13 |
Notes
- Oil-based capsules depend heavily on co-ingested fat; absorption can drop 30–50% fasted.
- Taken with ≥10 g fat, absorption approaches liposomal levels.
- 25(OH)D half-life ≈ 2–3 weeks; plateau reflects steady-state accumulation.
- Micellar/emulsified forms are pre-solubilized; ~30–40% higher absorption fasted vs. plain oil; gap largely closes with fat.
- No robust RCT evidence of faster 25(OH)D rise vs. plain D3 at equivalent doses once fat intake is controlled.
- Phospholipid envelope enables direct lymphatic uptake; partially bypasses gut metabolism; fat-independent.
- Early-rise data from small studies; clinical significance vs. plain D3 at therapeutic doses not yet fully established.
- Calcifediol (Rayaldee, Hidroferol) is already 25-hydroxylated — absorbed like any fat-soluble molecule and does not require hepatic conversion.
- Bypassing the liver's CYP2R1/CYP27A1 step is the key pharmacokinetic advantage over cholecalciferol in acute settings.
- Used in the Castillo et al. COVID-19 RCT (Córdoba); also the form recommended by some SCCM vitamin D working group discussions for rapid ICU repletion. Soft-gel formulation (Hidroferol) achieves faster peak than extended-release Rayaldee.
- Calcitriol is a small lipophilic molecule; also available as IV formulation for critical care bypass of all conversion steps.
- Short half-life makes calcitriol unsuitable for rebuilding 25(OH)D stores; acts directly on VDR without CYP27B1 activation.
- Hypercalcemia risk is significant with calcitriol — calcium and phosphate monitoring required. Best reserved for renal failure patients (who cannot activate calcifediol) or true emergencies where speed outweighs risk.
- Soft-gel Hidroferol formulation (widely available in Spain, used in the Castillo COVID trial) achieves a faster peak than the extended-release Rayaldee capsule approved in the US — same molecule, very different pharmacokinetics.
The above was made by Claude AI, May 2026
Related in VitaminDWiki
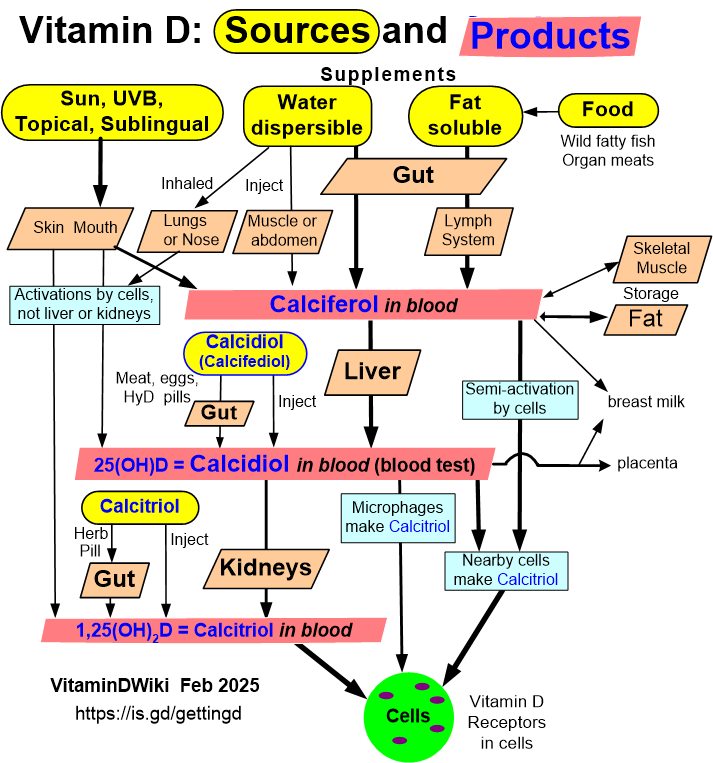
- Getting Vitamin D into your blood and cells has the following chart
Calcitriol
Liposomal (used by vitaminDWiki, very low cost)
- Liposomal is better than standard Vitamin D in 10 ways
- Liposomal Vitamin D raises blood levels 5X faster
- Mercury problems might be reduced by Liposomal Glutathione or Vitamin D
- Vitamin D: liposomal and nanoemulsion forms - Chat-GPT
- Liposomal Vitamin D3 compared with Calcidiol(Calcifediol)
Nanoemulsion (swish in mouth for fast response)
- Nanoemulsion Vitamin D is faster and better - many studies
- Nanoemulsion, nanoliposome, and conventional Vitamin D compared
Gut-Friendly
- Gut-Friendly Vitamin D
- Water-dispersible forms of vitamins A, D, E and K are better
- Water-dispersible Vitamin D may be gut-friendly (Cystic Fibrosis) – RCT
Inhaled (response in < 10 minutes?. especially good for lungs and nose