When to start Vitamin D after European births - UK 180 days, many 6-31 days, the rest 1-5 days
Variations in infant and childhood vitamin D supplementation programs across Europe and factors influencing adherence.
Endocr Connect. 2017 Sep 18. pii: EC-17-0193. doi: 10.1530/EC-17-0193. [Epub ahead of print]
Uday S1, Kongjonaj A2, Aguiar M3, Tulchinsky T4, Hoegler W5.
1 S Uday, Endocrinology and Diabetes, Birmingham Women's and Children's NHS Foundation Trust, Birmingham, B15 2TG, United Kingdom of Great Britain and Northern Ireland.
2 A Kongjonaj, MEAL specialist, Save the children international , Albania, United Kingdom of Great Britain and Northern Ireland.
3 M Aguiar, Health Economics, University of Birmingham, Birmingham, United Kingdom of Great Britain and Northern Ireland.
4 T Tulchinsky, Hebrew University of Jerusalem Braun School of Public Health and Community Medicine, Jerusalem, Israel.
5 W Hoegler, University of Birmingham, Birmingham, United Kingdom of Great Britain and Northern Ireland Wolfgang.Hogler@bch.nhs.uk.
📄 Download the PDF from VitaminDWiki
Graphics in the PDF
BACKGROUND:
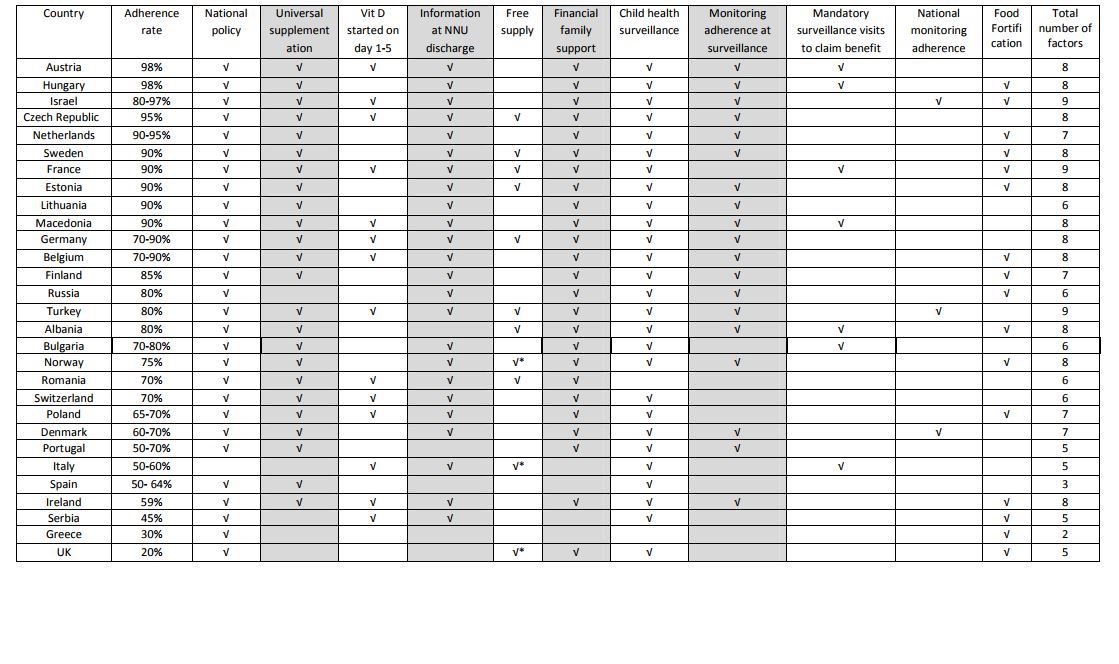
Nutritional rickets is a growing global public health concern despite existing prevention programs and health policies. We aimed to compare infant and childhood vitamin D supplementation policies, implementation strategies and practices across Europe and explore factors influencing adherence.
METHODS:
European Society for Paediatric Endocrinology Bone and Growth Plate Working Group members and other specialists completed a questionnaire on country-specific vitamin D supplementation policy and child healthcare programs, socioeconomic factors, policy implementation strategies, and adherence. Factors influencing adherence were assessed using Kendall's tau-b correlation coefficient.
RESULTS:
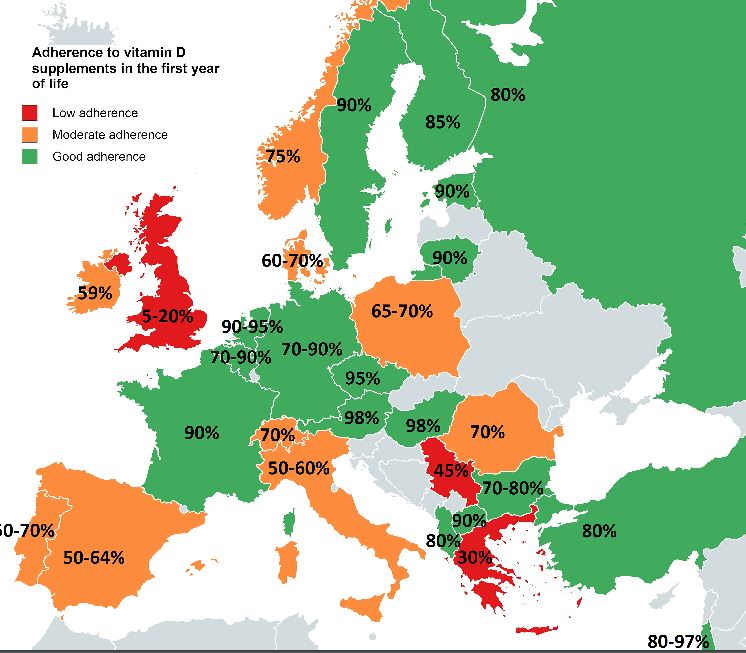
Responses were received from 29 of 30 European countries (97%). Ninety-six per cent had national policies for infant vitamin D supplementation. Supplements are commenced on day 1-5 in 48% (14/29) of countries, day 6-21 in 48% (14/29); only the UK (1/29) starts supplements at 6 months. Duration of supplementation varied widely (6 months to lifelong in at-risk populations). Good (≥80% of infants), moderate (50-79%) and low adherence (<50%) to supplements was reported by 59% (17/29), 31% (9/29) and 10% (3/29) of countries, respectively. UK reported lowest adherence (5-20%). Factors significantly associated with good adherence were universal supplementation independent of feeding mode (p=0.007), providing information at neonatal unit (NNU) discharge (p=0.02), financial family support (p=0.005); monitoring adherence at surveillance visits (p=0.001) and the total number of factors adopted (p<0.001).
CONCLUSIONS:
Good adherence to supplementation is a multi-task operation that works best when parents are informed at birth, all babies are supplemented and adherence monitoring is incorporated into child health surveillance visits. Implementation strategies matter for delivering efficient prevention policies.
PMID: 28924002 DOI: 10.1530/EC-17-0193