Small vitamin D doses provide small benefits for acute respiratory infections – Meta-analysis
Vitamin D supplementation to prevent acute respiratory infections: a systematic review and meta-analysis of aggregate data from randomised controlled trials - March 2021
www.thelancet.com/diabetes-endocrinology DOI:https://doi.org/10.1016/S2213-8587(21)00051-6
David A Jolliffe, PhD; Prof Carlos A Camargo Jr, MD; John D Sluyter, PhD; Mary Aglipay, MSc
Prof John F Aloia, MD; Davaasambuu Ganmaa, PhD
Background
A 2017 meta-analysis of data from 25 randomised controlled trials (RCTs) of vitamin D supplementation for the prevention of acute respiratory infections (ARIs) revealed a protective effect of this intervention. We aimed to examine the link between vitamin D supplementation and prevention of ARIs in an updated meta-analysis.
Methods
For this systematic review and meta-analysis, we searched MEDLINE, Embase, the Cochrane Central Register of Controlled Trials, Web of Science, and the ClinicalTrials.gov registry for studies listed from database inception to May 1, 2020. Double-blind RCTs of vitamin D3, vitamin D2, or 25-hydroxyvitamin D (25[OH]D) supplementation for any duration, with a placebo or low-dose vitamin D control, were eligible if they had been approved by a research ethics committee, and if ARI incidence was collected prospectively and prespecified as an efficacy outcome. Studies reporting results of long-term follow-up of primary RCTs were excluded. Aggregated study-level data, stratified by baseline 25(OH)D concentration and age, were obtained from study authors. Using the proportion of participants in each trial who had one or more ARIs, we did a random-effects meta-analysis to obtain pooled odds ratios (ORs) and 95% CIs to estimate the effect of vitamin D supplementation on the risk of having one or more ARIs (primary outcome) compared with placebo. Subgroup analyses were done to estimate whether the effects of vitamin D supplementation on the risk of ARI varied according to baseline 25(OH)D concentration (<25 nmol/L vs 25·0–49·9 nmol/L vs 50·0–74·9 nmol/L vs >75·0 nmol/L), vitamin D dose (daily equivalent of <400 international units [IU] vs 400–1000 IU vs 1001–2000 IU vs >2000 IU), dosing frequency (daily vs weekly vs once per month to once every 3 months), trial duration (≤12 months vs >12 months), age at enrolment (<1·00 years vs 1·00–15·99 years vs 16·00–64·99 years vs ≥65·00 years), and presence versus absence of airway disease (ie, asthma only, COPD only, or unrestricted). Risk of bias was assessed with the Cochrane Collaboration Risk of Bias Tool. The study was registered with PROSPERO, CRD42020190633.
Findings
We identified 1528 articles, of which 46 RCTs (75 541 participants) were eligible. Data for the primary outcome were obtained for 48 488 (98·1%) of 49 419 participants (aged 0–95 years) in 43 studies. A significantly lower proportion of participants in the vitamin D supplementation group had one or more ARIs (14 332 [61·3%] of 23 364 participants) than in the placebo group (14 217 [62·3%] of 22 802 participants), with an OR of 0·92 (95% CI 0·86–0·99; 37 studies; I2=35·6%, pheterogeneity=0·018). No significant effect of vitamin D supplementation on the risk of having one or more ARIs was observed for any of the subgroups defined by baseline 25(OH)D concentration. However, protective effects of supplementation were observed in trials in which vitamin D was given in a daily dosing regimen (OR 0·78 [95% CI 0·65–0·94]; 19 studies; I2=53·5%, pheterogeneity=0·003), at daily dose equivalents of 400–1000 IU (0·70 [0·55–0·89]; ten studies; I2=31·2%, pheterogeneity=0·16), for a duration of 12 months or less (0·82 [0·72–0·93]; 29 studies; I2=38·1%, pheterogeneity=0·021), and to participants aged 1·00–15·99 years at enrolment (0·71 [0·57–0·90]; 15 studies; I2=46·0%, pheterogeneity=0·027). No significant interaction between allocation to the vitamin D supplementation group versus the placebo group and dose, dose frequency, study duration, or age was observed. In addition, no significant difference in the proportion of participants who had at least one serious adverse event in the vitamin supplementation group compared with the placebo group was observed (0·97 [0·86–1·07]; 36 studies; I2=0·0%, pheterogeneity=0·99). Risk of bias within individual studies was assessed as being low for all but three trials.
Interpretation
Despite evidence of significant heterogeneity across trials, vitamin D supplementation was safe and overall reduced the risk of ARI compared with placebo, although the risk reduction was small. Protection was associated with administration of daily doses of 400–1000 IU for up to 12 months, and age at enrolment of 1·00–15·99 years. The relevance of these findings to COVID-19 is not known and requires further investigation.
📄 Download the PDF from VitaminDWiki
Meta-analysis was updated (but only 7 of the 40 trials used >2,000 IU) - Feb 2025
But the meta-analysis continued to average them all together - even trials using just 400 IU
https://doi.org/10.1016/S2213-8587(24)00348-6
VitaminDWiki comment and other studies
Of the 1500 trials to chose from,
most of the trials selected by this meta-analysis used <2,000 IU
about 20% of the trials were too short (<3 months) to expect any response to non-bolus doses
Infectious Disease typically not treated if use less than 4000 IU vitamin D daily– review Oct 2014
Asthma treated by monthly 100,000 IU of Vitamin D if person had very low levels – RCT Feb 2021
Acute respiratory tract infections not reduced by Vitamin D if already have a good level – Jan 2021
Those with Asthma or COPD had half the response to Vitamin D – March 2020
- Wonder if those prone to RTI have less response as well
All asthma problems reduced after 1 year of Vitamin D – Nov 2017
- 100,000 IU injection followed by 5,000 IU weekly
RTI – Feel much better if increase vitamin D level above 40 ng (4000 IU) – RCT Sept 2015
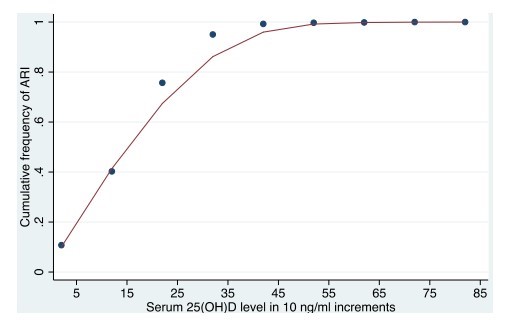
Respiratory Infection associated with vitamin D less than 40 ng – March 2015 which has the following chart
Breathing Meta-analysis
This list is automatically updated
{category}
20 studies in Breathing with non-daily Intervention
This list is automatically updated
{category}
Breathing items with ACUTE in title
This list is automatically updated
{LIST()}