Respirator track infections reduced when raise Vitamin D levels above 30 ng
Vitamin D and airway infections: a European perspective.
Eur J Med Res. 2016 Mar 24;21:14. doi: 10.1186/s40001-016-0208-y.
Zittermann A1, Pilz S2, Hoffmann H3, März W4,5,6.
 See also VitaminDWiki
* Breathing **category listing has items along with related searches**
* Respiratory Tract Infection visits 2.5 less likely with vitamin D: Pregnancy 2000 IU, Infant 800 IU – RCT Oct 2014
* Largest cause of infant deaths is respiratory infections, which is associated with low vitamin D – April 2011
* Respiratory infections (RTI) cut in half by 20,000 IU weekly vitamin D if initially deficient – RCT March 2015
* Respiratory tract infection eliminated in 36 percent of people by 4000 IU of Vitamin D – RCT Sept 2015
* Lower respiratory tract infections in children associated with Low Vitamin D – meta-analysis May 2016
* RTI – Feel much better if increase vitamin D level above 40 ng (4000 IU) – RCT Sept 2015
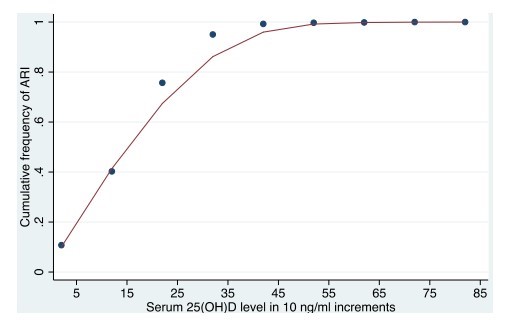
* Chart shows that there are very very few RTI for those individuals getting > 35 nanograms
*
See also VitaminDWiki
* Breathing **category listing has items along with related searches**
* Respiratory Tract Infection visits 2.5 less likely with vitamin D: Pregnancy 2000 IU, Infant 800 IU – RCT Oct 2014
* Largest cause of infant deaths is respiratory infections, which is associated with low vitamin D – April 2011
* Respiratory infections (RTI) cut in half by 20,000 IU weekly vitamin D if initially deficient – RCT March 2015
* Respiratory tract infection eliminated in 36 percent of people by 4000 IU of Vitamin D – RCT Sept 2015
* Lower respiratory tract infections in children associated with Low Vitamin D – meta-analysis May 2016
* RTI – Feel much better if increase vitamin D level above 40 ng (4000 IU) – RCT Sept 2015
* Chart shows that there are very very few RTI for those individuals getting > 35 nanograms
* 
📄 Download the PDF from VitaminDWiki
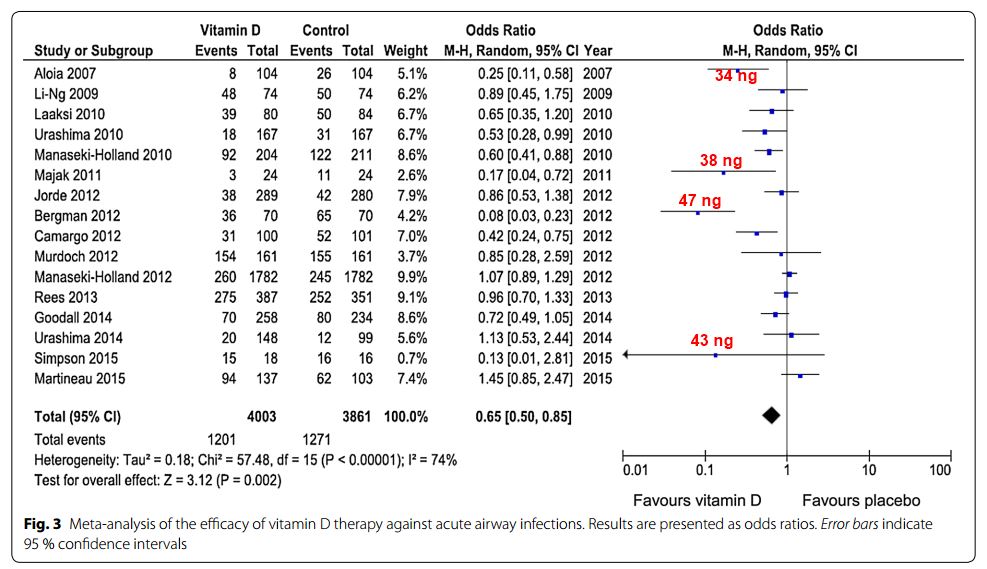
Vitamin D has immuno-modulatory properties, and deficient levels of circulating 25-hydroxyvitamin D (<30 nmol/l) may contribute to increased risk of infectious illnesses. This narrative review summarises data on vitamin D status in Europe and updates results of randomised controlled trials (RCTs) regarding vitamin D and airway infections such as tuberculosis (TB) and acute upper respiratory tract infection. In Europe, the prevalence of vitamin D deficiency is up to 37% in the general population and up to 80% in nursing home residents and non-European immigrants. Half of TB patients have a migration background. While results of RCTs do not support the concept of beneficial adjunctive effects of vitamin D supplements in anti-TB treatment [odds ratio (OR) = 0.86; 95% CI 0.62-1.19], the few published RCTs on the prophylaxis of TB suggest some protective vitamin D effects in individuals with deficient circulating 25-hydroxyvitamin D levels. Regarding acute respiratory tract infection, RCTs indicate a significant risk reduction by vitamin D supplements [OR = 0.65; 95% confidence interval (CI) 0.50-0.85]. There is evidence that daily administration is more effective than high-dose bolus administration [OR = 0.48 (95% CI 0.30-0.77) vs. OR = 0.87 (95% CI 0.67-1.14)] and that individuals with deficient or insufficient (30-50 nmol/l) circulating 25-hydroxyvitamin D levels benefit most. Several vitamin D effects on innate immunity may explain these protective effects. In summary, there is possible evidence from RCTs for protective vitamin D effects on TB and likely evidence for protective effects on acute airway infection. Since vitamin D deficiency is prevalent in Europe, especially in institutionalised individuals and non-European immigrants, daily oral vitamin D intake, e.g. 1000 international units, is an inexpensive measure to ensure adequate vitamin D status in individuals at risk.
PMID: 27009076 PMCID: PMC4806418 DOI: 10.1186/s40001-016-0208-y