12 Vitamin D experts - summary of video -May 2026
3+ hour Video on Vimeo
Summary by James Lyons-Weiler
James Lyons-Weiler, PhD — President, IPAK / IPAK-EDU
The statistical error underlying the current Recommended Dietary Allowance (RDA) and Tolerable Upper Intake Level (UL) for vitamin D was identified by Dr. Lyons-Weiler as the root cause of the policy failure. The Institute of Medicine (IOM) used study-level averages — not individual-level data — to infer what percentage of the population would be protected at a given dose. This is a fundamental misapplication of statistics called regression to the mean. Study averages compress variance. Population individuals do not. The inference that 97.5% of individuals are protected at the current RDA cannot be derived from averages of study populations. The error is not contested in the literature. It has simply never been corrected in policy.
- - Aluminum Hydroxide (in some vaccines) reduces vitamin D levels Claude AI: too little to make a difference
He further noted that aluminum hydroxide — the adjuvant used in multiple vaccines in the pediatric schedule, including Tdap administered during pregnancy — is known in the pharmacological literature to reliably induce asthma in animal models without additional antigen exposure, and causes hypophosphatemia, which is mechanistically linked to functional vitamin D deficiency. He committed to publishing a technical report on the aluminum hydroxide–vitamin D deficiency connection and called on HHS, NIH, and CDC to fund studies on autoimmunity and asthma risk from vaccine adjuvants during pregnancy. He also noted that a CDC-affiliated researcher, Frank DeStefano, published a study showing a strong association between Tdap vaccination in children and asthma risk — a finding that was attacked rather than investigated.
Dr. Michael Holick — Professor of Medicine, Boston University School of Medicine; 900+ publications
Dr. Holick provided the policy history. The 2010 IOM report set the UL at 4,000 IU/day — a fourfold increase from the previous 1,000 IU/day UL, which he characterized as a landmark acknowledgment that prior limits were wrong. However, the 2024 Endocrine Society guidelines reverted to the IOM’s population model rather than a medical model, assuming a healthy, vitamin D-sufficient baseline that does not reflect clinical reality.
Key findings Dr. Holick presented:
Vitamin D sufficiency (25-hydroxyvitamin D of_ at least 34 ng/mL) was associated with a 54% reduced likelihood of COVID-19_ infection in a dataset of over 190,000 Quest Diagnostics patient samples.
Hospital patients who were vitamin D sufficient at admission had a 67% reduced overall odds of death from COVID-19, and an 82% reduced odds if they were also normal weight.
Blood levels of 40–50 ng/mL are associated with maximum mortality benefit, per Garland’s data. Achieving that level requires 4,000–5,000 IU/day.
Hunter-gatherer populations maintain blood levels of 40–50 ng/mL naturally through sun exposure — this is the evolutionarily normal range.
10,000 IU/day has been demonstrated safe in healthy adults in studies he conducted with the late Dr. Robert Heaney.
The D2d study, initially reported as negative for diabetes prevention, showed a 76% three-year absolute risk reduction from prediabetes to diabetes in participants who achieved blood levels of at least 50 ng/mL versus those at 20–29 ng/mL.
The 2024 guidelines make no recommendations for obesity, recommend only 600 IU/day for pregnant women despite evidence supporting much higher doses, and explicitly advise against routine screening.
His bottom line: vitamin D deficiency is a disease of neglect. He recommends a minimum of 2,000 IU/day for adults, 1,000 IU/day for children, with testing to confirm adequacy.
Dr. William Grant — Founder, Sunlight Nutrition and Health Research Center; epidemiologist
Dr. Grant presented observational evidence across eight of the top ten causes of death in the United States, using data from large prospective cohort studies and ecological analyses. He and colleagues found that 25-hydroxyvitamin D concentrations above 30 ng/mL significantly reduce disease burden for conditions accounting for approximately 90% of all U.S. deaths in 2021–2022.
Specific findings:
- - Cardio, Colon Cancer,Stroke, Dementia, Kidney, Mortality, Diabetes, Hill’s Criteria
Cardiovascular disease: approximately twofold increased risk at 25-hydroxyvitamin D below 8 ng/mL versus sufficient levels.
Colorectal cancer: approximately 25% reduction for high versus low 25-hydroxyvitamin D, consistent with Garland et al. findings going back to 1974.
Stroke: approximately 60% reduction in risk for those with levels above 30 versus below 20 ng/mL at one-year follow-up.
Dementia: over twofold increased risk at five-year follow-up for those with levels below 20 versus above 30 ng/mL.
Chronic kidney disease: approximately 30% reduction in new-onset CKD in patients with diabetes (UK Biobank data, 12.1-year median follow-up).
Mortality: consistent with Garland et al., blood levels of 40–50 ng/mL are associated with maximum survival benefit.
Prediabetes-to-diabetes conversion: the Tufts University study showed significant risk reduction at levels above 50 ng/mL versus below 30 ng/mL.
Dr. Grant noted that mean U.S. 25-hydroxyvitamin D levels (NHANES data) rose from approximately 25 ng/mL in 2000–2001 to approximately 31 ng/mL by 2022–2024, likely attributable to observational research reaching the public — not to clinical guideline changes or RCT findings. He called this the “golden age of vitamin D” research.
He addressed causality directly, citing A.B. Hill’s 1965 criteria presented to the Royal Society of Medicine. For vitamin D, the criteria of strength of association, consistency across populations, temporality, biological gradient, plausibility, coherence, experimental verification, and analogy are substantially met across the literature. He further noted that an Israeli study linking severe COVID-19 outcomes to low vitamin D status was retracted in 2025 on procedural grounds — a retraction he characterized as serving pharmaceutical interests rather than scientific integrity.
Dr. Edward Giovannucci — Professor of Nutrition and Epidemiology, Harvard T.H. Chan School of Public Health
- - 9 reasons RCTs find null results
Dr. Giovannucci provided the most rigorous defense of observational evidence and the most detailed analysis of why randomized controlled trials (RCTs) produce false negatives for vitamin D. He identified nine documented factors that push RCTs toward null results when studying nutrients — factors that do not apply to drug trials, where baseline status is not a confounder.
His key points from the VITAL trial (26,000 participants, 2,000 IU/day, approximately five years):
The trial enrolled a population whose mean baseline 25-hydroxyvitamin D was approximately 30 ng/mL — already at the sufficiency threshold identified in observational data. The intervention raised the mean to approximately 42 ng/mL. Observational data predict no additional benefit in that range for cardiovascular disease and fracture endpoints, which is exactly what VITAL found.
Cancer mortality (pre-specified endpoint): a 25% reduction was observed after excluding the first two years. When endpoints were verified through medical records, a statistically significant 37% reduction in total cancer mortality was found.
A meta-analysis of three trials using daily (not bolus) dosing found a statistically significant 13% reduction in total cancer mortality.
Autoimmune disease: a 22% reduction in confirmed autoimmune diseases; nearly 40% reduction when excluding the first two years — highly statistically significant.
Diabetes: in prediabetic participants across 10 trials, highly statistically significant reversion to normal glycemia favored vitamin D supplementation.
BMI interaction: across four separate analyses, benefits were consistently concentrated in lean participants (BMI under 25), with highly significant interactions — a 44% reduction in metastatic cancer and a 24% reduction in invasive cancer among lean participants in VITAL. This is not chance.
Long-term toxicity: no evidence of hypercalcemia or any adverse effects from attaining 40–50 ng/mL over up to six years of follow-up.
On Mendelian randomization: Dr. Giovannucci conducted a review of over 100 Mendelian randomization studies on vitamin D. Positive signals — consistent with a causal effect of higher vitamin D on outcomes — were found for cardiovascular disease, cancer, autoimmune conditions, diabetes, cognitive function, and several other endpoints. Because these signals are based on genetic determinants of vitamin D status rather than lifestyle, they are not confounded by the factors that complicate observational epidemiology.
Dr. Bruce Hollis — Professor of Pediatrics (emeritus), Medical University of South Carolina
Dr. Hollis has conducted FDA-monitored clinical trials of vitamin D in pregnancy since the early 2000s. His group was the first required to obtain an Investigational New Drug (IND) number from the FDA to study 4,000 IU/day in pregnant women — a requirement he described as absurd for a nutrient and illustrative of the institutional bias baked into the system.
Key findings:
- - 4,000 IU during pregnancy. Should reduce preterm birth
In a randomized trial of 400, 2,000, and 4,000 IU/day in pregnant women, post-hoc analysis revealed statistically significant reductions in preeclampsia, preterm labor, and gestational diabetes at higher doses — findings that were initially attacked when presented in 2009.
A study conducted in India (2015, Clinical Endocrinology) in a uniformly vitamin D-deficient population showed massive decreases in gestational diabetes, preeclampsia, and preterm labor in the supplemented versus placebo group. This study was rejected by the New England Journal of Medicine, JAMA, and the BMJ.
A subsequent study in Iran with similar design showed dramatic reductions in a composite of adverse birth outcomes, with hazard ratios that were highly statistically significant. Also rejected by major journals.
Human breast milk is a poor source of vitamin D when the mother is deficient. His group demonstrated that 6,400 IU/day given to lactating mothers produced sufficient vitamin D in breast milk to fully nourish the nursing infant without separate infant supplementation — a finding available to pediatricians that has never been incorporated into official AAP recommendations.
There is currently no approved treatment for preterm labor in the United States. A drug (17-hydroxyprogesterone) that was given preliminary FDA approval and marketed for years — after the company was acquired for $700 million — was eventually pulled by the FDA for failure to demonstrate efficacy. Vitamin D supplementation, by contrast, has randomized trial evidence supporting its protective effect in high-risk populations and has been consistently ignored.
Dr. Carol Wagner — Neonatologist and Professor of Pediatrics, Medical University of South Carolina
Dr. Wagner framed vitamin D in pregnancy not as a single nutrient intervention but as part of a developmental system operating across maternal, placental, and fetal biology. This framing, recently articulated in an American Journal of Clinical Nutrition editorial, changes the research question from “does this dose prevent this complication” to “what does it mean for the developing system to have adequate versus inadequate vitamin D across the entire developmental window.”
Key points:
- - Preterm birth 2X high risk if low vit D, need 40-60 ng
Vitamin D deficiency compounds existing racial and socioeconomic health disparities in birth outcomes — vitamin D-deficient populations had nearly double the rate of preterm birth in studies she cited, following a dose-response relationship that strengthens biological plausibility.
Maternal vitamin D status affects human milk composition, including components that shape the infant immune system and microbiome.
Higher early-life vitamin D status has been associated with better neurodevelopmental outcomes across multiple cohorts.
From an evolutionary perspective, what constitutes physiologic normalcy during pregnancy is a serum level consistent with sustained outdoor activity — approximately 40–60 ng/mL — not the 20 ng/mL currently deemed sufficient by the IOM.
Dr. Scott Weiss — Professor of Medicine, Harvard Medical School; Principal Investigator, VDART
Dr. Weiss designed and led the Vitamin D Antenatal Asthma Reduction Trial (VDART), the first large RCT of prenatal vitamin D supplementation and childhood asthma. He used 4,000 IU/day because Dr. Hollis held the FDA IND for that dose; higher doses would have required a separate IND application.
Key findings:
Often need >4,000 IU during pregnancy to get > 30 ng, start before conception, 99% of pregnancies are now <60 ng
In VDART, 70% of pregnant women receiving 4,000 IU/day achieved serum levels of at least 30 ng/mL. Yet 30% of obese women in that group remained insufficient even at 4,000 IU/day.
The primary intention-to-treat analysis did not reach statistical significance for the primary endpoint, but a pre-specified analysis adjusting for baseline level and time of enrollment recovered the 50% reduction in childhood asthma and wheeze seen in prior observational studies.
The window for fetal airway development is weeks 5–10 of pregnancy. VDART enrolled at 10–18 weeks. Ideally, supplementation should begin at or before conception.
Contamination of the control group — participants who were already vitamin D sufficient at enrollment and continued supplementing — is a fundamental confounding feature of nutrient RCTs not present in drug trials.
99–100% of pregnant women in the United States have 25-hydroxyvitamin D levels below 60 ng/mL. The optimal serum target for asthma prevention, based on VDART pharmacokinetic analysis, is 60 ng/mL — not 30.
Preterm birth and preeclampsia in VDART were found to increase the risk of offspring asthma and impaired neurodevelopmental outcomes, linking adverse pregnancy outcomes to long-term child health in a mechanistic chain that vitamin D supplementation can interrupt.
Dr. Hooman Mirzakhani — Assistant Professor of Medicine, Harvard Medical School; Faculty, Channing Division, Brigham and Womens Hospital
Dr. Mirzakhani presented a framework for the optimal design of the next prenatal vitamin D supplementation trial, drawing on lessons from VDART. He identified why prior trials have failed to detect effects: wrong timing, insufficient dose, failure to account for BMI, failure to achieve target levels early, and reliance on a single dose without stratification.
Key design principles he outlined:
- - Start Vitamin D before conception if possible, >4,000 IU if obese
Ideally, enrollment should begin preconception or before 20 weeks gestation.
Baseline 25-hydroxyvitamin D should be measured in all participants.
Dosing should be stratified by BMI — obese women require substantially higher doses.
Intent-to-treat analysis should be primary, but pre-specified stratified analyses by BMI and achieved level are essential.
Cumulative vitamin D exposure across pregnancy — measured as area under the curve — is a stronger predictor of outcomes than endpoint level alone. In VDART pharmacokinetic analysis, each standard deviation above 30 ng/mL in cumulative exposure reduced offspring asthma and wheeze by 25% at enrollment and by 70% at six years.
Primary maternal outcomes (preterm birth, preeclampsia) and primary child outcomes (asthma, neurodevelopment) may require separate trial designs — a pragmatic maternal-focused trial and a more mechanistic maternal-child factorial design.
Dr. Sunil Wimalawansa — Director, Cardiometabolic and Endocrine Institute; former Professor of Medicine, Rutgers University
Dr. Wimalawansa presented 15 key clinical and mechanistic principles that explain why vitamin D research produces inconsistent results and why a one-size-fits-all dose cannot work.
Key points:
- - Cofactors needed, genes often restrict how much D gets to cells, need 50-80 ng, need 70-90 IU/kg/day, more if in poor in health or obese
Vitamin D is a threshold nutrient, not a pharmacological agent. Its dose-response is shallow. Adding more beyond sufficiency confers no additional benefit.
Vitamin D is a network nutrient — it requires cofactors including magnesium, omega-3 fatty acids, and vitamin K2. Some cases of apparent vitamin D resistance are actually magnesium deficiency.
During active disease, infection, or hospitalization, vitamin D utilization increases dramatically. Even a patient admitted with normal vitamin D levels can become deficient within days during acute illness, extending hospital stay and increasing costs.
Two people with the same serum vitamin D level can have entirely different biological outcomes due to genetic variants in the vitamin D binding protein and vitamin D receptor, and due to cofactor variability.
The target serum range that addresses 99.5% of vitamin D-responsive disorders is 50–80 ng/mL. The current IOM target of 20 ng/mL was designed solely for rickets and osteomalacia prevention and has no relevance to immune, metabolic, neurological, or cardiovascular health.
Vitamin D dosing should be individualized based on body weight. Non-obese patients require approximately 70–90 IU/kg/day. Obese patients require proportionally more.
The U.S. healthcare system is driven by a pharmaceutical model that treats symptoms and ignores root causes. A shift to root-cause medicine — addressing micronutrient deficiencies as primary drivers of chronic disease — is necessary for meaningful reform.
Nutrition receives approximately two hours of instruction in most U.S. medical curricula. Vitamin D receives approximately 20 minutes.
Dr. Leigh Frame — Chief Medical Officer, Recondite Consulting; Co-Founder, GW Resiliency and Wellbeing Center
Dr. Frame focused on physiological stress states — hospitalization, surgery, acute illness — as natural experiments that reveal the consequences of low vitamin D status most clearly.
Key findings:
Lower vitamin D status is associated with increased respiratory infections, longer hospital stays, higher ICU severity, and worse critical illness outcomes.
For surgical patients, vitamin D status predicts wound healing, dehiscence risk, surgical site infection, rehabilitation capacity, and overall recovery trajectory.
Insufficient vitamin D impairs adaptive immune response to vaccination — individuals with low vitamin D produce fewer antibodies and lower viral titers after vaccination than those with sufficient levels.
Rescue dosing after an acute event is likely insufficient. The immune system requires sustained, proactive vitamin D sufficiency; correction after crisis cannot reverse early dysregulation.
Her call to action: vitamin D status assessment should be as routine in acute care as glucose, fluid balance, and oxygenation monitoring.
Dr. Richard Cheng, MD, PhD — Editor-in-Chief, Orthomolecular Medicine News Service; Board Director, Riordan Clinic
Dr. Cheng presented a systems medicine framework for understanding why individual responses to vitamin D supplementation vary so dramatically. His framework — Integrative Orthomolecular Systems Medicine — extends Linus Pauling’s orthomolecular principles by integrating nutrient biology with metabolic health, biological barriers, inflammation, and physiological resilience.
Key points:
Vitamin D simultaneously influences immunity, inflammation, metabolism, endothelial function, mitochondrial activity, neuroendocrine signaling, and gene expression. Treating it as a single-target nutrient misrepresents its biology.
Biological barrier integrity — gut, lung, vascular endothelium, skin, blood-brain barrier — is substantially dependent on vitamin D. When barriers become dysfunctional, chronic inflammation and immune dysregulation follow.
- - For identical D levels, stressors and genes make for different outcomes
Two individuals with identical serum vitamin D levels may have entirely different outcomes based on inflammation status, metabolic health, cofactor adequacy, diet quality, sleep, stress, and genetics. Vitamin D does not function in isolation.
The question systems medicine asks is not “which nutrient affects which disease” but “what impairs resilience, what increases inflammatory burden, what disrupts metabolic flexibility.”
Rising cancer rates in adults under 50 — up approximately 80% over the past 30 years — and the rise of autism spectrum disorder cannot be explained by genetics. Environmental and nutritional drivers are primary. Focusing on genetics alone is scientifically insufficient and practically useless for population-level prevention.
Dr. Beth Sanford, DNP — Director of Education and Clinical Practice, Grassroots Health; President, North Dakota Nurses Association
Dr. Sanford presented the Vitamin D Risk Ecology — a practical public health framework that maps individual, population, and environmental risk factors to guide clinical decision-making and policy at every level of the socioecological model.
Key practical contributions:
Vitamin D risk is shaped by geography (latitude, seasonal UVB availability), population vulnerability (pregnancy, darker skin tones, occupational indoor exposure, obesity), and individual biology. Population-level and individual-level interventions must be designed in recognition of all three.
Documented symptoms that justify clinical coding for vitamin D deficiency include fatigue, generalized weakness, sleep disturbance, cognitive impairment, headache, mood dysregulation, neuromuscular pain, post-surgical pain, and frequent infections. Documentation enables insurance reimbursement for testing and supplementation.
Grassroots Health has developed evidence-based dose calculators incorporating body weight, current serum level, and target serum level that allow clinicians to generate individualized loading and maintenance dose recommendations in minutes.
- - Vit D levels crashed after sepsis, Alaska and North Dakota have Vitamin D resolutions
Her mother — maintained at approximately 60 ng/mL — dropped to 30 ng/mL within 30 days during a sepsis episode, demonstrating the rapidity of depletion under physiological stress.
Alaska and North Dakota are the only two U.S. states with vitamin D resolutions. She challenged panelists and their contacts to advocate for similar resolutions in their own states.
Final policy recommendations: update guidelines to regionally specific sun exposure recommendations; add vitamin D protocols to WIC, cancer prevention programs, workforce health, and military health initiatives; require standardized research design using the Heaney criteria; and integrate vitamin D science into all existing public health programming rather than treating it as a separate initiative.
Robin Whittle — Independent Researcher and Commentator (audience)
Mr. Whittle, commenting from the audience, made the case that Dr. Wimalawansa’s body-weight-based dosing recommendations — the only peer-reviewed body-weight-stratified vitamin D dosing framework in the literature — should replace the RDA concept entirely for population-wide recommendations. His analysis indicated that achieving 50 ng/mL in the top 2.5% of U.S. body weights (approximately 133 kg / 290 lbs, consistent with Class 3 obesity) would require approximately 18,000 IU/day under the RDA framework, making the RDA an absurd and misleading construct for this nutrient.
CONSENSUS POSITIONS OF THE PANEL
All speakers agreed on the following:
The current federal vitamin D guidelines (IOM 2010 and Endocrine Society 2024) are not adequate for clinical care and should not be used as the basis for treatment decisions.
The minimum sufficient serum 25-hydroxyvitamin D level for health — beyond bone — is at minimum 40 ng/mL and optimally 50–80 ng/mL for most conditions.
10,000 IU/day is safe for adults, as demonstrated by multiple long-term trials. The current UL of 4,000 IU/day is overly conservative.
Vitamin D dosing must account for body weight, BMI, and baseline serum level. A universal dose cannot be derived without these inputs.
Testing is essential. The recommendation against routine screening in the 2024 Endocrine Society guidelines is inconsistent with the evidence and harmful.
Pregnancy and early infancy represent the most critical windows for intervention.
*Preterm birth, *preeclampsia, *gestational diabetes, *childhood asthma, and *neurodevelopmental outcomes
are all modifiable through adequate maternal vitamin D status.
The failure to update policy despite available evidence reflects systemic resistance — economic, institutional, and regulatory — not scientific uncertainty.
- - SINGLE HIGHEST-PRIORITY POLICY ACTION: update Federal guideline
When asked what one HHS action would have the greatest immediate impact, the near-unanimous answer was:
Update the official federal vitamin D guidelines — the government-recommended serum sufficiency threshold and the RDA — to reflect current evidence. As long as outdated numbers appear on official federal websites, clinicians and the public will default to them regardless of what else is communicated.
Related in VitaminDWiki
- 5 Critical Analyses of the 2024 Endocrine Society Guideline on Vitamin D
- Is 50 ng of vitamin D too high, just right, or not enough
- US admits math mistake was made in 2010 in estimating Vitamin D, but will not change recommendations
- 21 reasons why doctors are reluctant to accept Vitamin D
- Consensus Vitamin D
- A drug that could reduce all these health problems is worth a Trillion dollars - video Holick
- Vitamin D: 40-70 ng is optimal, sometimes more is needed - Grant, Sunil, Pawel, Cheng
3 of the experts with video presentations on current page - Optimum
- Vitamin D is needed for human fertility – goal is 50 ng
- More than 30 ng of vitamin D is needed for many diseases
*World's Top Authors in Vitamin D, VDR, Vitamin K, Omega-3, etc
4 of the top 10 Vitamin D authors were in this video - Vitamin D is unprofitable, so medicine ignores it
- Gut-Friendly Vitamin D
not mentioned in videos, but needed by 30% of people with low vitamin D problems - Response to Vitamin D - many studies
- Top 10 chronic health problems of children, women, pregnancies, seniors, and darker skins are fought by Vitamin D
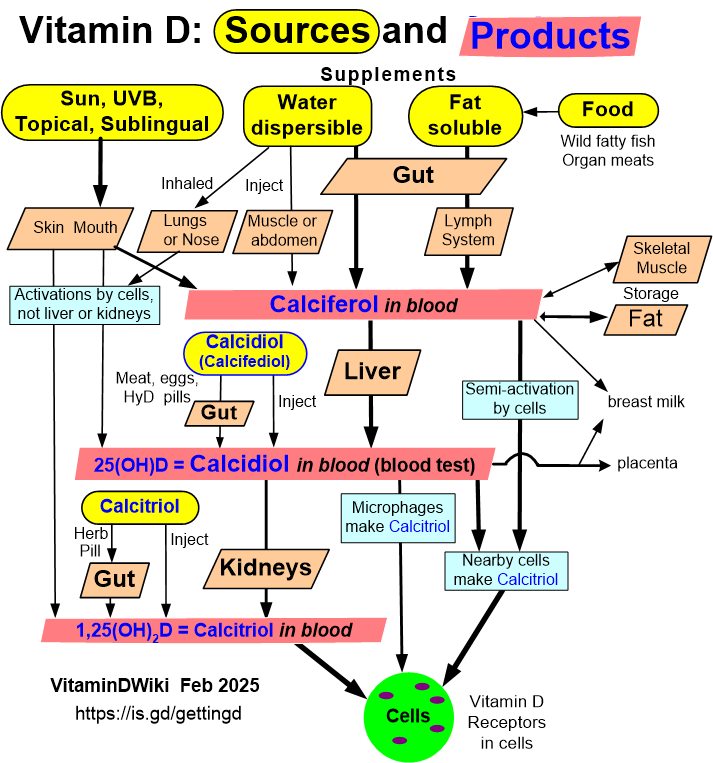
- Getting Vitamin D into your blood and cells
Stressors & Genetics
- 20+ chronic stressors result in poor health (most are fought by Vitamin D)
- Genetics
- Benefits of Vitamin D often limited by genes
See also: tags at the bottom of this (and most other) VitaminDWiki pages