Late sepsis deaths ~1.7X more likely if vitamin D below 12 ng - need-for-speed
Vitamin D at hospital admission as an independent predictor of outcome of sepsis patients: Results of a secondary analysis from a "Need-Speed" trial prospective cohort
European Journal of Internal Medicine, June 2026, https://doi.org/10.1016/j.ejim.2026.107025
Pier Paolo Sainaghi, Manuela Rizzi, Stelvio Tonello, et al. — on behalf of the Delivida-NeedSpeed Study Group
Summary by Claude - June 2026
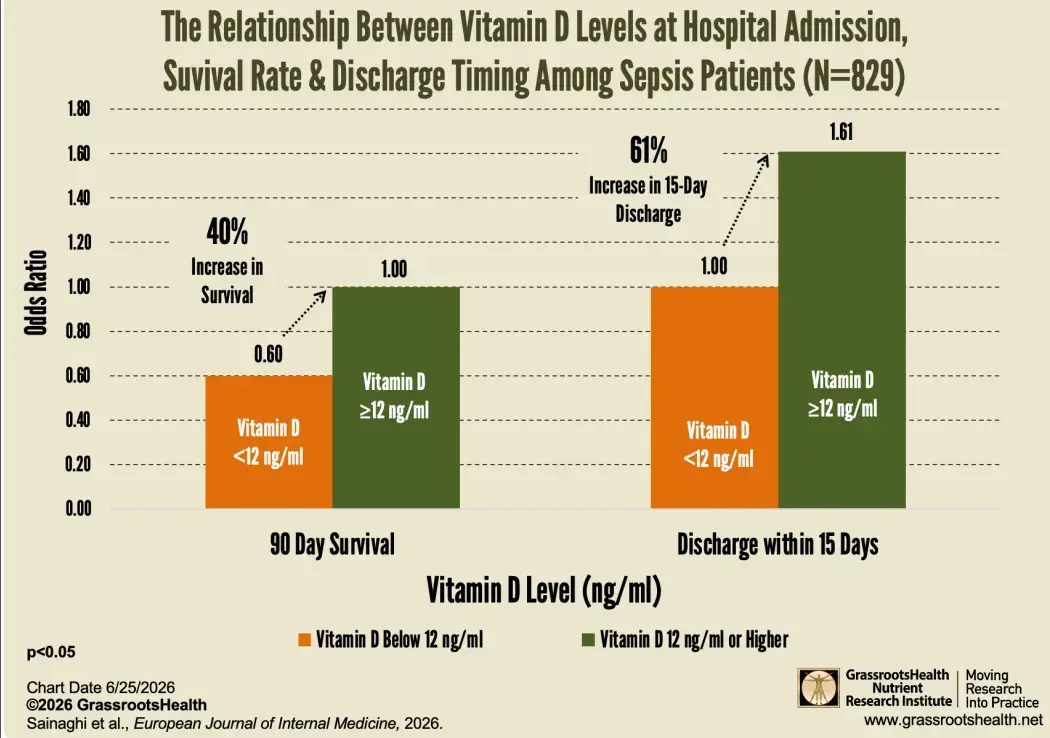
Among 829 mostly very elderly hospital patients (median age 81) with confirmed sepsis, those with higher vitamin D at admission were more likely to survive and recover faster — and the level still predicted outcome after adjusting for age, illness severity (NEWS2), comorbidity (Charlson index), CRP, lactate, and procalcitonin.
This is a secondary analysis of a prospective multicenter observational cohort (five Italian hospitals), not a treatment trial. A single baseline 25(OH)D was measured by chemiluminescence. The population was severely deficient across the board — median 25(OH)D just 11.2 ng/mL (28 nmol/L) — so this study compares degrees of deficiency, not deficiency versus sufficiency.
Key results: 7-day mortality showed no link to vitamin D, and 30-day mortality lost significance after adjustment. Only 90-day mortality and discharge alive within 15 days held up. Patients dying within 90 days had a median of 9.6 ng/mL versus 12.0 ng/mL in survivors. Using a 12 ng/mL cut-off, those at or above it had about 40% lower odds of 90-day death (OR 0.596, 95% CI 0.407–0.874) — equivalently, patients below 12 ng/mL had about 1.7X the odds of 90-day death and ~61% higher odds of early discharge (OR 1.606, 1.174–2.196).
The authors are candid that vitamin D alone discriminates poorly (AUC 0.579) and is best used alongside existing risk scores, as a marker of immune reserve/frailty — and that the late-outcome signal fits the "post-sepsis" PICS syndrome.
What this does NOT show / limitations: This is association, not causation — low vitamin D may simply flag frailer, less-mobile, poorly-nourished patients. Endpoints were not pre-specified (exploratory). The 12 ng/mL threshold is internal to this cohort and unvalidated, and is not a health target. A single admission level can be depressed by acute inflammation, and no PTH, frailty, nutrition, or supplementation data were available. Crucially, this study does not show that giving vitamin D improves sepsis outcomes; the cited ICU supplementation trials (VITdAL-ICU, PETAL/VIOLET) were conflicting/null and were not aimed at elderly septic patients.
Review of study at GrassrootsHealth
Related in VitaminDWiki
- Sepsis is both prevented and treated by Vitamin D - many studies
- 1.5X increased infection, sepsis, and death if in ICU with low vitamin D - Meta-analysis
- Sepsis 2X-3X more likely if poor Vitamin D Receptor – meta-analysis
- Sepsis is treated by Vitamin D if you are low - meta-analysis 2025
- Sepsis mortality greater in Black than White children (low vitamin D)
- Sepsis is fought by Vitamin D in 9 ways
- Severe sepsis may be prevented by 400,000 IU of vitamin D – RCT 2023
- Vitamin D for Sepsis prevention
Need for Speed with Sepsis, etc.
- Vitamin D can start working in minutes — if you pick the right form slowest to fastest forms:
fat-soluble,
water dispersible
dispersible dissolved in water then swished in mouth
nanoemulsion
Nanoemulsion swished in mouth/topical
Calcitriol - Fast responses to Vitamin D – loading dose, nanoemulsion and Calcifediol
- Nanoemulsion Vitamin D is faster and better - many studies