800 IU and 20 ng is enough vitamin D, need RCT
Optimal Vitamin D Status: A Critical Analysis on the Basis of Evidence-Based Medicine
The Journal of Clinical Endocrinology & Metabolism August 1, 2013 vol. 98 no. 8 E1283-E1304
Roger Bouillon, roger.bouillon@med.kuleuven.be
Natasja M. Van Schoor,
Evelien Gielen,
Steven Boonen Deceased May 20, 2013
Chantal Mathieu,
Dirk Vanderschueren and
Paul Lips
Clinical and Experimental Endocrinology (R.B., C.M., D.V.), KU Leuven, Departments of Endocrinology and Laboratory Medicine, UZ Leuven, 3000 Leuven, Belgium; Department of Internal Medicine, Endocrine Section, and
Department of Epidemiology and Biostatistics (N.M.V.S., P.L.), EMGO Institute for Health and Care Research, VU University Medical Centre, 1007 MB Amsterdam, The Netherlands; and
Gerontology and Geriatrics (E.G., S.B.), KU Leuven and Geriatric Medicine, UZ Leuven, 3000 Leuven, Belgium
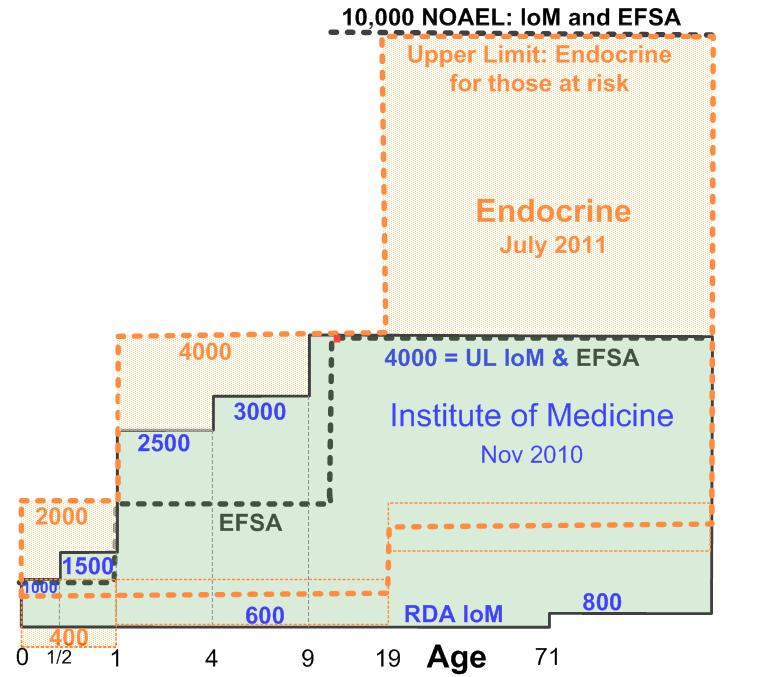
Context: Public health authorities around the world recommend widely variable supplementation strategies for adults, whereas several professional organizations, including The Endocrine Society, recommend higher supplementation.
Methods: We analyzed published randomized controlled clinical trials to define the optimal intake or vitamin D status for bone and extraskeletal health.
Conclusions: The extraskeletal effects of vitamin D are plausible as based on preclinical data and observational studies. However, apart from the beneficial effects of 800 IU/d of vitamin D3 for reduction of falls in the elderly, causality remains yet unproven in randomized controlled trials (RCTs). The greatest risk for cancer, infections, cardiovascular and metabolic diseases is associated with 25-hydroxyvitamin D (25OHD) levels below 20 ng/mL. There is ample evidence from RCTs that calcium and bone homeostasis, estimated from serum 1,25-dihydroxyvitamin D and PTH, calcium absorption, or bone mass, can be normalized by 25OHD levels above 20 ng/mL. Moreover, vitamin D supplementation (800 IU/d) in combination with calcium can reduce fracture incidence by about 20%. Such a dose will bring serum levels of 25OHD above 20 ng/mL in nearly all postmenopausal women. Based on calculations of the metabolic clearance of 25OHD, a daily intake of 500–700 IU of vitamin D3 is sufficient to maintain serum 25OHD levels of 20 ng/mL.
Therefore, the recommendations for a daily intake of 1500–2000 IU/d or serum 25OHD levels of 30 ng or higher for all adults or elderly subjects, as suggested by The Endocrine Society Task Force, are premature .
Fortunately, ongoing RCTs will help to guide us to solve this important public health question.
Abreviations:
BMD = bone mineral density
BMI = body mass index
CI = confidence interval
CKD = chronic kidney disease
CL = confidence limit
COPD = chronic obstructive pulmonary disease
FGF23 = fibroblast growth factor 23
HR = hazard ratio
1,25(OH)2D = 1,25-dihydroxyvitamin D
25OHD = 25-hydroxyvitamin D
OR = odds ratio
RCT = randomized controlled trials
RR = relative risk
VDR = vitamin D receptor.
See also VitaminDWiki
Vitamin D Recommendations around the world - IU and ng which includes the following
- Proof that Vitamin D Works has the following data - the above study seems to ignore the data
- {include}
- Overview Pregnancy and vitamin D which has the following summary
- {include}