Vitamin D, Omega-3, Butyrate etc., should help if taking GLP-1 for weight loss
Vitamin D and GLP-1 drugs
GLP-1 receptor agonists (semaglutide — Ozempic/Wegovy; tirzepatide — Mounjaro/Zepbound; liraglutide — Saxenda) now drive weight loss at a population scale. The weight comes off fast, and fast weight loss by any route carries musculoskeletal and micronutrient costs — and the quality of the weight lost (fat vs lean mass) is the real clinical issue.
The model that ties this together: vitamin D acts as a conditioning / permissive factor — it amplifies the body's response to the two interventions that matter most here. In deficient people on caloric restriction, repletion amplifies fat loss; in combination with adequate protein, it enables muscle synthesis. GLP-1 users sit squarely in both conditions (caloric restriction + reliance on protein to hold lean mass + elevated deficiency risk from reduced intake). So the relevant question for GLP-1 users is not "does vitamin D cause weight loss" but "does vitamin D improve the quality of the weight lost" — and the conditioned evidence says plausibly yes.
The core problem GLP-1 drugs create
- Lean mass loss. Lean body mass can account for 15–40% of total weight lost on GLP-1 therapy, with better estimates around 20–30% — comparable to, and sometimes slightly better than, diet-only weight loss. The SURMOUNT-1 DXA substudy (Look et al., 2025) reported ~10.9% total lean-mass loss over 72 weeks on tirzepatide.
- Bone loss. The most rigorous bone-specific trial (Hansen et al., eClinicalMedicine 2024; 52 weeks, semaglutide 1.0 mg vs placebo, adults at increased fracture risk) found a 2.6% drop in hip BMD and 2.1% at the lumbar spine, with increased bone resorption and no compensatory rise in formation. The FDA semaglutide label notes possible increased fracture risk in older adults and women.
- Reduced intake. Sharp appetite suppression means less food — and a higher risk of vitamin and mineral shortfalls, including the fat-soluble vitamins.
Where vitamin D plausibly helps
Starting point — almost every obese GLP-1 candidate begins insufficient. This is the fact the rest of the page leans on. At the strict deficiency cutoff (25(OH)D <20 ng/mL), roughly 30–40% of obese adults qualify (NHANES: ~29% deficiency overall, with obesity a significant predictor). But at the insufficiency threshold most vitamin D researchers use (<30 ng/mL / <75 nmol/L), the majority of all US adults fall short (only ~34.5% exceed 75 nmol/L), and for the obese specifically — driven further down by volumetric dilution and adipose sequestration — the below-sufficiency fraction is plausibly 80–90%+. Practically: assume a GLP-1 candidate is insufficient until a test says otherwise. That makes the supplemented-vs-replete distinction below largely academic for this population — almost all of them are in the group that stands to benefit from repletion.
1. Bone — the strongest and most urgent angle (Tier 1 rationale)
This is more clinically established than the muscle angle and deserves to lead. Vitamin D + calcium is foundational, evidence-backed bone-health support independent of GLP-1s. Against a documented 2–3%/year BMD loss on these drugs, maintaining sufficiency is the floor below which any bone-protection plan should not fall. Practitioner consensus is already converging on resistance training + adequate protein + calcium + vitamin D3 + baseline DXA as standard of care for GLP-1 therapy — not as extras.
- Established: vitamin D's role in calcium absorption and bone mineralization.
- Gap: no trial has tested whether vitamin D supplementation specifically blunts GLP-1-associated BMD loss. The rationale is strong; the direct evidence is extrapolated.
2. Muscle / lean mass — preservation and gain when paired with protein (Tier 1–2)
The mechanistic case is real. Myocyte-specific VDR-knockout mice show reduced proportional lean mass (70% vs 78%), reduced grip strength, and reduced voluntary running (Girgis et al., J Cachexia Sarcopenia Muscle 2019). Loss of VDR function in myotubes lowers mitochondrial respiration and ATP output.
And the human RCT evidence for the combination is strong, not merely suggestive. The PROVIDE study (Verlaan/Bauer et al., Clin Nutr 2017; n=380 sarcopenic older adults, 13 weeks, no exercise) found that a vitamin D + leucine-enriched whey protein drink added appendicular muscle mass and improved chair-stand performance — with the muscle gain seen mainly in those who reached sufficient 25(OH)D. The mechanism: vitamin D acts synergistically with leucine and insulin to stimulate muscle protein synthesis. Related RCTs (e.g., 4,000 IU for 4 months in insufficient elderly) show similar muscle gains. So in the deficient/insufficient, the D+protein combination demonstrably builds muscle — it does not merely slow loss.
Read the PROVIDE "baseline sufficiency required" finding correctly — it is a dosing lesson, not a barrier. PROVIDE used only 800 IU; over 13 weeks that is too little to replete a deficient person fast enough to cross the functional threshold within the trial, so only those who started sufficient responded. The actionable conclusion is therefore replete adequately and quickly (consider a loading dose), then maintain — not "deficient people can't benefit." The weight-loss trials below, which used 25,000–100,000 IU/month, did replete deficient obese people and did see benefit. The unifying principle across all of it is reaching sufficiency, by whatever dose that takes.
The conditioning caveat (narrowed): vitamin D monotherapy in an already-replete person does not reliably add muscle — it works by enabling the anabolic response to protein. That is exactly why it matters for GLP-1 users: near-universal insufficiency in the obese (see below) means almost all of them start below the threshold, with intake and protein simultaneously suppressed by the drug.
- Application to GLP-1: GLP-1 users are under caloric restriction with reduced protein intake and elevated deficiency risk — the precise profile in which D+protein preserves and can rebuild lean mass. This reframes vitamin D from "slows muscle loss" to "enables the protein-driven lean-mass preservation that is the goal of GLP-1 musculoskeletal care."
- Gap: no RCT has yet tested the D+protein combination specifically during GLP-1 therapy. The case is extrapolated from the sarcopenia/caloric-restriction literature — but that literature includes positive RCTs, not just observational signals.
3. Quality of weight loss — amplified fat loss in deficient dieters (Tier 2 — conditional)
This is the angle your pushback surfaced, and it belongs in the page. In vitamin D-deficient people on a low-calorie diet, repletion is associated with substantially greater weight and fat loss:
- Vigna et al. (J Am Coll Nutr 2021, retrospective/observational, n=405 insufficient workers on a moderately-low-calorie diet): supplemented groups lost 4.1–4.5 kg vs 1.2 kg untreated; waist circumference fell up to −6.2 cm vs −3.2 cm.
- The widely-cited "quadruples" trial (n≈400 deficient obese/overweight on low-calorie diet): 100,000 IU/month → ~12 lb loss, 25,000 IU/month → ~8 lb, diet-only control → ~2.6 lb.
The honesty counterweight : the Perna 2019 meta-analysis of 11 RCTs (947 subjects) found vitamin D supplementation reduced BMI (−0.32 kg/m²) and waist circumference (−1.42 cm) but did not significantly change body weight (−0.43 kg, p=0.17) — in trials that mostly used neither caloric restriction nor high-dose/infrequent dosing. So the weight-loss amplification is real but conditional on deficiency + caloric restriction (and possibly on infrequent high-dose regimens). For GLP-1 users — who are deficiency-prone and under caloric restriction — those conditions are met, which is what makes the angle relevant rather than generic.
- Gap: no trial has tested whether vitamin D enhances fat loss (or fat-vs-lean partitioning) during GLP-1 therapy.
4. Falls in older users (Tier 2)
Older adults on GLP-1s face a compounding risk: lean-mass loss + BMD loss + (if deficient) impaired neuromuscular function. Vitamin D's fall-reduction signal is real but limited to deficient/older populations and inconsistent in the replete. Where it applies, it sits on the same at-risk group that bone and muscle concerns flag.
5. The status paradox during weight loss (Tier 2 — the distinctive mechanistic angle)
This is the part most coverage gets wrong, and where VitaminDWiki can add value. Two opposing forces act on vitamin D status during GLP-1 weight loss:
- Downward: reduced food intake lowers vitamin D (and fat-soluble vitamin) input.
- Upward: fat loss tends to raise serum 25(OH)D. In a systematic review, 18 of 23 non-supplementing weight-loss trials documented an increase in 25(OH)D with weight/fat loss — consistent with reversal of the volumetric dilution (and/or sequestration) that depresses 25(OH)D in obesity (Drincic et al., 2012; Walsh et al.).
Net effect is genuinely uncertain and likely depends on the balance between intake drop and fat-loss magnitude. Two practical implications:
- A "normal" serum 25(OH)D during rapid weight loss may be partly a measurement artifact of fat mobilization rather than true repletion — tissue availability and total-body stores are a separate question.
- This argues for measuring 25(OH)D before and during GLP-1 therapy rather than assuming either depletion or sufficiency.
- Gap: no study has tracked the intake-loss vs fat-release balance prospectively in GLP-1 users specifically. The exercise-mobilization pathway (Bath RCT program) suggests fat-stored D can be released, but the GLP-1 context is unstudied.
What vitamin D does NOT do
This section is deliberately narrowed to what the evidence actually supports as a limit — overstating the limits is as damaging to credibility as overstating the benefits.
- It is not a standalone weight-loss drug. In replete people, and in RCTs without caloric restriction, it does not produce significant weight loss (Perna 2019 meta-analysis). Its weight effect appears only in deficient people who are also dieting.
- It does not build muscle as monotherapy in a replete person — its muscle effect is a synergy that requires adequate protein (and is concentrated in the deficient/insufficient). It enables the anabolic response; it does not substitute for protein.
- It is not a reason to forgo a baseline DXA, protein targeting, or resistance training — those remain the backbone of GLP-1 musculoskeletal care.
- It does not replace or reduce the need for the GLP-1 drug itself, and does not treat obesity on its own.
Research gaps
- No RCT of vitamin D for muscle or bone preservation during GLP-1 therapy.
- No prospective tracking of the intake-reduction vs fat-mobilization balance on 25(OH)D in GLP-1 users.
- Optimal dosing during rapid fat loss is unknown — volumetric-dilution reversal could change the dose needed to maintain a target level.
- Whether tissue/functional vitamin D availability tracks serum 25(OH)D during active fat loss is unresolved.
Practical takeaways
- Treat vitamin D sufficiency as a prerequisite that amplifies the two interventions GLP-1 users depend on — adequate protein (muscle) and caloric restriction (fat loss) — not as an optional add-on.
- Replete early and adequately — don't under-dose. The positive effects appear once 25(OH)D is brought to sufficiency; the PROVIDE "baseline sufficiency" result reflects an 800 IU dose too weak to replete the deficient in time, not an inability of deficient people to respond. Consider a loading dose, then maintain.
- Measure 25(OH)D at baseline and periodically; interpret mid-weight-loss values cautiously given fat-mobilization effects.
- The case is strongest and most mainstream for bone, RCT-supported (in combination with protein) for muscle, conditional-but-real for quality of weight loss in deficient dieters, and most under-studied for the status paradox.
References
- Look et al. SURMOUNT-1 DXA substudy. Diabetes, Obesity and Metabolism, 2025. (Tirzepatide ~10.9% lean-mass loss over 72 weeks.)
- Hansen MS et al. Once-weekly semaglutide vs placebo in adults with increased fracture risk: a randomised, double-blinded, two-centre, phase 2 trial. eClinicalMedicine, 2024. (Hip BMD −2.6%, lumbar −2.1%.)
- Kushner et al. (STEP investigators). Bone mineral density and body composition in people with obesity treated with semaglutide 2.4 mg. Obesity (Silver Spring), 2023.
- Girgis CM et al. Mice with myocyte deletion of vitamin D receptor have sarcopenia and impaired muscle function. J Cachexia Sarcopenia Muscle, 2019.
- Verlaan S, Bauer JM et al. (PROVIDE study). Sufficient 25(OH)D and protein intake required to increase muscle mass in sarcopenic older adults. Clin Nutr, 2017. (D + leucine-whey protein, 13 wk, no exercise → muscle gain; baseline sufficiency required.)
- Vigna L et al. Effects of vitamin D supplementation on outcome of low-calorie diet in workers with obesity/overweight. J Am Coll Nutr, 2021. (Observational; −4.5 kg supplemented vs −1.2 kg untreated, deficient dieters.)
- "Quadruples weight loss" trial (deficient obese/overweight on low-calorie diet; 100,000 IU/mo → ~12 lb, 25,000 IU/mo → ~8 lb, control → ~2.6 lb). Conference-presented; see VitaminDWiki page.
- Perna S. Is vitamin D supplementation useful for weight loss programs? A systematic review and meta-analysis of RCTs. Medicina (Kaunas), 2019. (11 RCTs; BMI −0.32, WC −1.42 cm, weight n.s. −0.43 kg — null in unselected trials without caloric restriction.)
- Vitamin D status modulates mitochondrial oxidative capacities in skeletal muscle. Communications Biology, 2022.
- Vitamin D and sarcopenia review. PMC (PMC12383353), 2025. (Supplementation benefit concentrated in deficient + protein/resistance-training contexts.)
- Drincic A et al. Volumetric dilution, rather than sequestration, best explains the low vitamin D status of obesity. Obesity (Silver Spring), 2012.
- Systematic review: change in 25(OH)D after weight loss (18/23 trials increased). ScienceDirect, 2014.
- "Mobilising vitamin D sequestered in adipose tissue in humans" — University of Bath RCT program (exercise-induced 25(OH)D release).
- ADA 85th Scientific Sessions (2025): BELIEVE trial (bimagrumab + semaglutide), muscle-preservation pharmacology.
Omega-3, Butyrate, Zinc, Magnesium etc. also help
Claude AI -June 2026
Related in VitaminDWiki
- The Potential Synergy Between Vitamin D and GLP-1 Medications for Enhanced Weight Loss
- 40% of weight loss from GLP-1 is from muscle loss (not so if lose weight with Vitamin D)
- Sarcopenia (muscle loss) fought by Vitamin D, exercise and protein - many studies
- Seniors can restore lost muscle (Sarcopenia) – first restore vitamin D, then exercise
- Overview Fractures and vitamin D
- Overview Obesity and Vitamin D
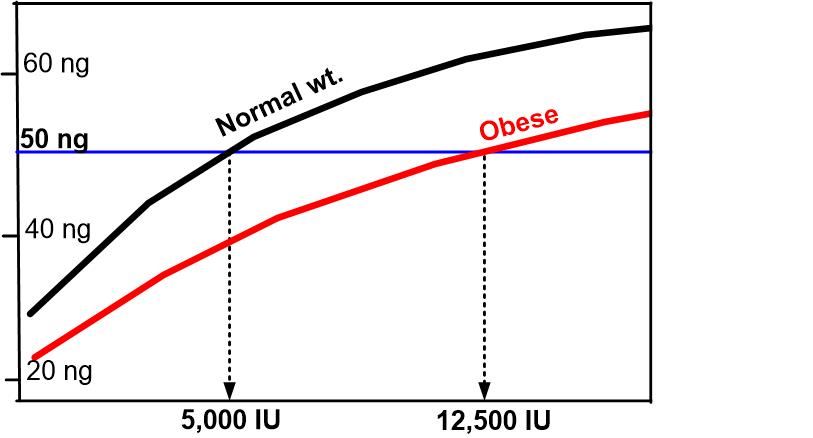
- Obese need 2X to 3X more vitamin D - has the following chart