Veiled Somali pregnant women in Sweden had low vitamin D and were weak
Physical performance and 25-hydroxyvitamin D: a cross-sectional study of pregnant Swedish and Somali immigrant women and new mothers.
BMC Pregnancy Childbirth. 2013 Dec 17;13(1):237.
Kalliokoski P, Bergqvist Y, Löfvander M.
BACKGROUND: Severe vitamin D deficiency can impair muscle strength. The study aims were to examine physical performance in the hands and upper legs, and analyze plasma 25-hydroxyvitamin D (25(OH)D) concentrations in women with presumably low (veiled, Somali-born) and high levels (unveiled, Swedish-born).
METHODS: Women (n=123, 58% Swedish) enrolled at a Swedish antenatal clinic, latitude 60 [degree sign] N, were recruited. Plasma 25(OH) D was analyzed, measured as nmol/L, then categorized as <10 = undetectable, 10-24, 25-49, 50-74 or >75. Muscle strength was tested: maximal hand grip strength (in Newtons, N), and upper leg performance (categorized as able/unable to perform squatting, standing on one leg, standing from a chair, and lifting their hips). Social and anthropometric data were collected. Non-parametric statistics tested the data for differences in their ability to perform the tests across 25(OH)D categories. Undetectable values (<10 nmol/L) were replaced with '9' in the linear correlation statistics. A final main effect model for grip strength (in N) was calculated using stepwise linear regression for independent variables: country of birth, 25(OH)D levels, age, height, weight, physical activity, lactation status, parity, and gestational age.
RESULTS:
Somali participants
(35%) had 25(OH)D levels of <10 nmol/L, and
90% had <25 nmol/L;
10% of Swedish participants had <25 nmol/L of 25(OH)D, and
54% had <50 nmol/L.
Somali women had a relatively weak grip strength compared with Swedish women: median
202 N (inter-quartile range 167-246) vs. median
316 N (inter-quartile range 278-359), respectively.
Somali women were also weak in upper leg performance:
73% were unable to squat,
29% unable to stand on one leg, and
21% could not lift their hips (not significant across 25(OH)D categories);
most Swedish women could perform these tests.
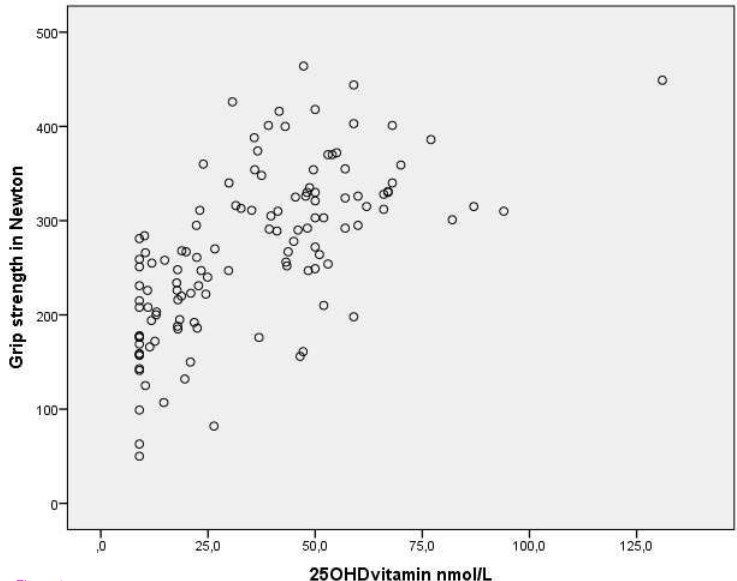
In the final model, grip strength (N) was significantly associated with 25(OH)D levels (B 0.94, p=0.013) together with Somali birth (B -63.9, p<0.001), age (B 2.5, p=0.02) and height (B 1.7, p=0.01)
CONCLUSIONS: Many Somali women had undetectable/severely low 25(OH)D concentrations and pronounced hand and upper leg weakness; grip strength was strongly associated with 25(OH)D. Maternity health care personnel should be aware of this increased frequency and manage care accordingly.

The higher the vitamin D, the stronger the grip


Biochemical osteomalacia during pregnancy or lactation: an observational study in Sweden - Feb 2026
BMC Pregnancy Childbirth. 2026 Feb 24;26(1):220. doi: 10.1186/s12884-026-08848-1.
Thomas Torstensson 1, Per Kristiansson 2, Paul Kalliokoski 2
BACKGROUND: Studies of osteomalacia during pregnancy and lactation are scarce. This is likely due to the hazards of performing X-ray in pregnancy, the inconvenience of the gold standard diagnostic procedure of bone marrow biopsy with histomorphometry and the lack of these resources in maternity health care. Another important reason is the lack of international consensus on how to diagnose osteomalacia clinically. Osteomalacia needs attention due to the limited number of modern studies on its prevalence and globalization, especially in some populations where migration to high latitudes with poor light conditions, as in Scandinavia, can heighten its prevalence. The aim of this study was to determine the prevalence of biochemical osteomalacia during pregnancy or lactation among Somali and Swedish women living in Sweden.
METHODS: This was an observational cohort study of 71 Swedish and 52 Somali pregnant or lactating women. Blood samples, self-report questionnaires and physical examination data were collected in late spring. The diagnostic criteria for biochemical osteomalacia were serum levels of a 25-hydroxy vitamin D3 (25(OH)D) concentration < 30 nmol/L, a parathyroid hormone (PTH) concentration > 6.9 pmol/L and an alkaline phosphatase (ALP) concentration > 1.8 ukat/L. The presence of clinical symptoms (grip weakness, leg weakness, a positive Trendelenburg test, fatigue, and pain) was used to reaffirm the diagnosis. RESULTS: The diagnostic criteria for biochemical osteomalacia were met by one Swedish woman 1/71 (1.4%) and 18/52 (34.6%) of all Somali women, of whom 1/71 (1.4%) and 16/52 (30.8%), respectively, had signs or symptoms reaffirming the diagnosis.
CONCLUSIONS: Women of Somali origin living at high altitudes are at high risk for vitamin D deficiency osteomalacia, but Swedish women may also suffer from this disease. These findings call for further studies on the prevalence of vitamin D deficiency, especially among groups at risk of vitamin D deficiency, because of the hidden disease burden. Establishing internationally accepted criteria for a noninvasive clinical diagnostic procedure for osteomalacia is imperative. TRIAL REGISTRATION: ClinicalTrials.gov Identifier: NCT02922803. Date of registration: September 28, 2016.
See also VitaminDWiki
Vitamin D improves muscle strength if deficient – meta-analysis - Oct 2010
Higher vitamin D during pregnancy associated with stronger hand grip at age 4 – Oct 2013
Muscle strength not increased by raising vitamin D to only 30 ng – RCT Aug 2012
More than 40 ng vitamin D for Athletes – July 2010 nice tables
Hypothesis: Why so many females in the Middle East are now Vitamin D Deficient
More hijab clothing may have resulted in 6X increase in Multiple Sclerosis in Tehran – May 2013
Dark skinned pregnant women far from equator were very vitamin D deficient – Sept 2012
Concealing clothing resulted in only 8 ng vitamin D – Feb 2011 France
Concealing Clothing in Canada: half the level of vitamin D in blood – May 2012
Hypothesis: Why so many females in the Middle East are now Vitamin D Deficient