ICU mortality reduced by non-oral vitamin D – meta-analysis
The Effect of Vitamin D Supplementation on Clinical Outcomes for Critically Ill Patients: A Systemic Review and Meta-Analysis of Randomized Clinical Trials
Front Nutr. 2021 May 4;8:664940. doi: 10.3389/fnut.2021.664940
Hejuan Shen 1 2, Yijun Mei 1 2, Kai Zhang 3, Xiaoya Xu 1 2
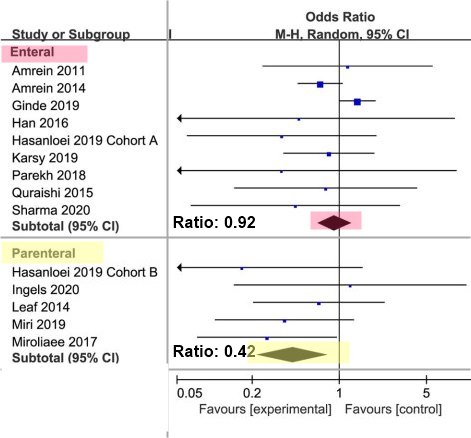
58% less mortality vs 8% for oral (Note: 8% was not statistically significant)
 1. Items in both categories Trauma-surgery and Loading Dose:
{category}
1. Injection category listing has items
1. Items in both categories Trauma-surgery and injection:
{category}
1. Items in both categories Trauma-surgery and Loading Dose:
{category}
1. Injection category listing has items
1. Items in both categories Trauma-surgery and injection:
{category}
📄 Download the PDF from VitaminDWiki
Purpose: Vitamin D deficiency is a common scenario in critically ill patients and has been proven to be associated with poor outcomes. However, the effect of vitamin D supplementation for critically ill patients remains controversial. Thus, we conducted a meta-analysis to evaluate the effect of vitamin D supplementation among critically ill patients.
Methods: Electronic databases PubMed, Embase, Scopus, and the Cochrane Library were searched for eligible randomized controlled trials between 2000 and January 2021. The primary outcome was overall mortality, and the secondary ones were the length of intensive care unit stay, the length of hospital stay, as well as the duration of mechanical ventilation. Subgroup analyses were performed to explore the treatment effect by type of admission, route of administration, dose of supplemented vitamin D, and the degree of vitamin D deficiency.
Results: A total of 14 studies involving 2,324 patients were finally included. No effect on overall mortality was found between vitamin D supplementation and control group [odds ratio (OR), 0.73; 95% CI, 0.52-1.03; I 2 = 28%]. The vitamin D supplementation reduced the length of intensive care unit stay [mean difference (MD), -2.25; 95% CI, -4.07 to -0.44, I 2 = 71%] and duration of mechanical ventilation (MD, -3.47; 95% CI, -6.37 to -0.57, I 2 = 88%).
In the subgroup analyses, the vitamin D supplementation for surgical patients (OR, 0.67; 95% CI, 0.47-0.94; I 2 = 0%) or through parenteral way (OR, 0.42 ; 95% CI, 0.22-0.82, I 2 = 0%) was associated with reduced mortality.
Conclusion: In critically ill patients, the supplementation of vitamin D has no effect on overall mortality compared to placebo but may decrease the length of intensive care unit stay and mechanical ventilation. Further trials are necessary to confirm our findings.