ICU death rate reduced 3X when a vitamin D injection changed the PTH
A Randomized Study of a Single Dose of Intramuscular Cholecalciferol in Critically Ill Adults.
Crit Care Med. 2015 Nov;43(11):2313-20. doi: 10.1097/CCM.0000000000001201.
Nair P1, Venkatesh B, Lee P, Kerr S, Hoechter DJ, Dimeski G, Grice J, Myburgh J, Center JR.
1Intensive Care Unit, St. Vincent's Hospital, Sydney, NSW, Australia. 2Faculty of Medicine, University of New South Wales, Sydney, NSW, Australia. 3Bone Biology Division, Garvan Institute for Medical Research, Sydney, NSW, Australia. 4Critical Care and Trauma Division, George Institute for Global Health, Sydney, NSW, Australia. 5Intensive Care Unit, Princess Alexandra Hospital, Brisbane, QLD, Australia. 6Intensive Care Unit, Wesley Hospital, Brisbane, QLD, Australia. 7University of Queensland, Brisbane, QLD, Australia. 8Departement of Anesthesiology, LMU, Munich, Germany. 9Intensive Care Unit, St. George Hospital, Sydney, NSW, Australia.
 The items which are in both Intervention and Trauma/Surgery are listed here
{category}
The items which are in both Intervention and Trauma/Surgery are listed here
{category}
OBJECTIVES:
To determine the effect of two doses of intramuscular cholecalciferol on serial serum 25-hydroxy-vitamin-D levels and on pharmacodynamics endpoints: calcium, phosphate, parathyroid hormone, C-reactive protein, interleukin-6, and cathelicidin in critically ill adults.
DESIGN:
Prospective randomized interventional study.
SETTING:
Tertiary, academic adult ICU.
PATIENTS:
Fifty critically ill adults with the systemic inflammatory response syndrome.
INTERVENTION:
Patients were randomly allocated to receive a single intramuscular dose of either 150,000 IU (0.15 mU) or 300,000 IU (0.3 mU) cholecalciferol.
MEASUREMENTS AND MAIN RESULTS:
Pharmacokinetic, pharmacodynamic parameters, and outcome measures were collected over a 14-day period or until ICU discharge, whichever was earlier. Prior to randomization, 28 of 50 patients (56%) were classified as vitamin D deficient. By day 7 after randomization, 15 of 23 (65%) and 14 of 21 patients (67%) normalized vitamin D levels with 0.15 and 0.3 mU, respectively (p=0.01) and by day 14, 8 of 10 (80%) and 10 of 12 patients (83%) (p=0.004), respectively.
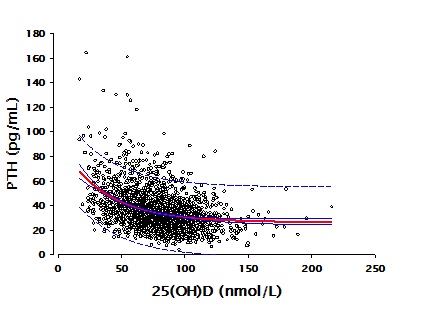
Secondary hyperparathyroidism was manifested in 28% of patients at baseline. Parathyroid hormone levels decreased over the study period with patients achieving vitamin D sufficiency at day 7 having significantly lower parathyroid hormone levels (p<0.01).
Inflammatory markers (C-reactive protein and interleukin-6) fell significantly over the study period.
Greater increments in 25-hydroxy-vitamin-D were significantly associated with greater increments in cathelicidin at days 1 and 3 (p=0.04 and 0.004, respectively). Although in-hospital mortality rate did not differ between the groups, patients who did not mount a parathyroid hormone response to vitamin D deficiency had a higher mortality (35% vs 12%; p=0.05) . No significant adverse effects were observed.
CONCLUSIONS:
A single dose of either dose of intramuscular cholecalciferol corrected vitamin D deficiency in the majority of critically ill patients. Greater vitamin D increments were associated with early greater cathelicidin increases, suggesting a possible mechanism of vitamin D supplementation in inducing bactericidal pleiotropic effects.
PMID: 26186566