Cystic Fibrosis not helped by 50,000 IU of Vitamin D taken twice a month – RCT
Vitamin D for the Immune System in Cystic Fibrosis (DISC): a double-blind, multicenter, randomized, placebo-controlled clinical trial.
Am J Clin Nutr. 2019 Feb 22. pii: nqy291. doi: 10.1093/ajcn/nqy291
Tangpricha V1,2,3,4, Lukemire J5, Chen Y5, Binongo JNG5, Judd SE6, Michalski ES1,2, Lee MJ1, Walker S3, Ziegler TR1,2,3,4, Tirouvanziam R3,7, Zughaier SM8, Chesdachai S1, Hermes WA1, Chmiel JF9, Grossmann RE10, Gaggar A11, Joseph PM12, Alvarez JA1,2,3.
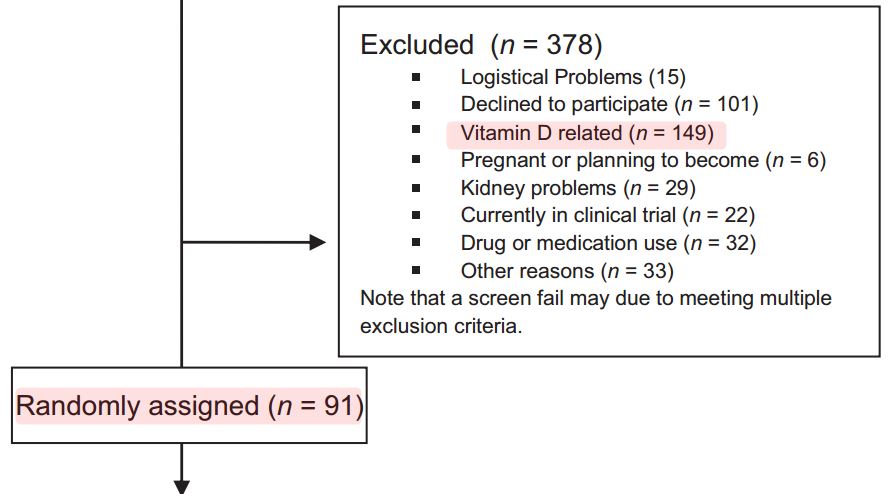 1.6X as many were rejected due to Vitamin D than were accepted (149 vs 91
Speculation: Those who were accepted tended to be those who had previously found that
standard Vitamin D without Magnesium did not help their CF
Cystic Fibrosis patients often have gut absorption problens,
so need higher doses or different forms of Vitamin D, such as:
* 50,000 IU weekly (or more frequent)
* Note: Founder of VitaminDWiki is taking 50,000 IU every 2 days (Feb 2019)
* 100,000 IU monthly (see below with CF)
* Gut-friendly (see below)
* Topical (see below)
* Have Vitamin D with evening meal (in gut longer increases response ~30%)
* Also take Magnesium (increases response ~30%)
* Perhaps also use inhaled form of Vitamin D
* * Cystic Fibrosis category listing has items *
* Cystic Fibrosis probably treated by Vitamin D (if use enough of the right type ) – Oct 2019
---
1. Overview Gut and vitamin D contains gut-friendly information
{include}
1.6X as many were rejected due to Vitamin D than were accepted (149 vs 91
Speculation: Those who were accepted tended to be those who had previously found that
standard Vitamin D without Magnesium did not help their CF
Cystic Fibrosis patients often have gut absorption problens,
so need higher doses or different forms of Vitamin D, such as:
* 50,000 IU weekly (or more frequent)
* Note: Founder of VitaminDWiki is taking 50,000 IU every 2 days (Feb 2019)
* 100,000 IU monthly (see below with CF)
* Gut-friendly (see below)
* Topical (see below)
* Have Vitamin D with evening meal (in gut longer increases response ~30%)
* Also take Magnesium (increases response ~30%)
* Perhaps also use inhaled form of Vitamin D
* * Cystic Fibrosis category listing has items *
* Cystic Fibrosis probably treated by Vitamin D (if use enough of the right type ) – Oct 2019
---
1. Overview Gut and vitamin D contains gut-friendly information
{include}
📄 Download the PDF from Sci-Hub via VitaminDWiki
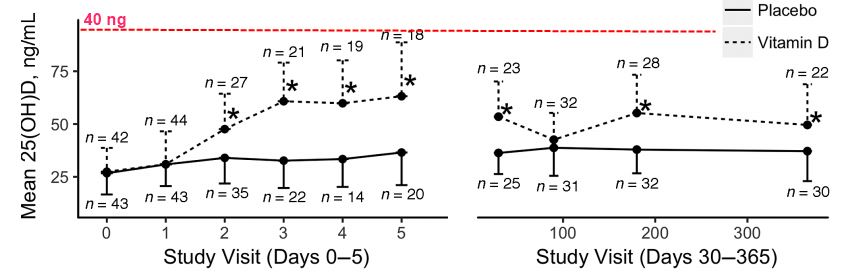
Left Chart: Poor response to 250,000 IU Loading Dose
CFers are known to have poor absorption of fat-soluable Vitamins (D, K, etc)
Most people with good guts would have ((Large dose of vitamin D (200,000 IU) lasts for about 100 days – Feb 2015
The effect of a single, large bolus of vitamin D in healthy adults over the winter and following year|>40 ng response to such a loading dose))
Right Chart: Poor response to 50,000 IU every 2 weeks Maintenance Dose
This would typically result in 40 ng/ml blood response
CFers clearly have far lower bio-availability to this oral vitamin D
BACKGROUND:
Patients with cystic fibrosis (CF) have increased risk of vitamin D deficiency owing to fat malabsorption and other factors. Vitamin D deficiency has been associated with increased risk of pulmonary exacerbations of CF.
OBJECTIVES:
The primary objective of this study was to examine the impact of a single high-dose bolus of vitamin D3 followed by maintenance treatment given to adults with CF during an acute pulmonary exacerbation on future recurrence of pulmonary exacerbations.
METHODS:
This was a multicenter, double-blind, placebo-controlled, intent-to-treat clinical trial. Subjects with CF were randomly assigned to oral vitamin D3 given as a single dose of 250,000 International Units (IU) or to placebo within 72 h of hospital admission for an acute pulmonary exacerbation, followed by 50,000 IU of vitamin D3 or an identically matched placebo pill taken orally every other week starting at 3 mo after random assignment. The primary outcome was the composite endpoint of the time to next pulmonary exacerbation or death within 1 y. The secondary outcomes included circulating concentrations of the antimicrobial peptide cathelicidin and recovery of lung function as assessed by the percentage of predicted forced expiratory volume in 1 s (FEV1%).
RESULTS:
A total of 91 subjects were enrolled in the study. There were no differences between the vitamin D3 and placebo groups in time to next pulmonary exacerbation or death at 1 y. In addition, there were no differences in serial recovery of lung function after pulmonary exacerbation by FEV1% or in serial concentrations of plasma cathelicidin.
CONCLUSIONS:
Vitamin D3 initially given at the time of pulmonary exacerbation of CF did not alter the time to the next pulmonary exacerbation, 12-mo mortality, serial lung function, or serial plasma cathelicidin concentrations. This trial was registered at clinicaltrials.gov as NCT01426256.