Child exposed to smoke is 1.5 X more likely to have low vitamin D
Tobacco smoke exposure is an independent predictor of vitamin D deficiency in US children
PLOS x https://doi.org/10.1371/journal.pone.0205342
Benjamin Udoka Nwosu Benjamin.Nwosu@umassmemorial.org , Philip Kum-Nji
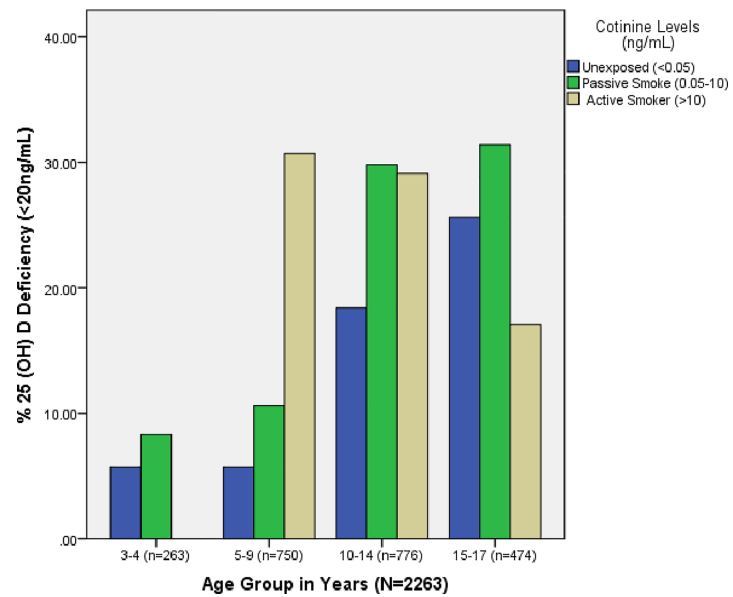
Age 5 - 9: 30% likely to have < 20 ng if a smoker
Age 10-14: 30% likely to have < 20 ng if smoker or second hand smoke
Age 15-17: 30% likely to have < 20 ng if second hand smoke but only 18% if a smoker seems strange
📄 Download the PDF from VitaminDWiki
Importance
The role of tobacco-smoke exposure on serum vitamin D concentration in US pediatric population is not known. We hypothesized that tobacco smoke exposure would increase the prevalence of vitamin D deficiency in US children.
Methods
Representative national data were accessed from the National Health and Nutrition Examination Survey (NHANES) 2009–2010 databank on 2,263 subjects of ages 3 to 17 years. Subjects were categorized into two groups based on their age: children, if <10 years; and youth if 10 to 17 years. Descriptive and multiple logistic regression analyses were conducted to determine the effect of serum cotinine-verified tobacco smoke exposure on vitamin D status after controlling for key sociodemographic confounders. Vitamin D deficiency was defined as 25(OH)D <20 ng/mL, insufficiency as 25(OH)D of 20–29.9 ng/mL, and sufficiency as 25(OH)D of ≥30 ng/mL. Tobacco smoke exposure status was defined by serum cotinine concentration as follows: unexposed and non-smoking (<0.05 ng/mL) and exposed (passive and active smokers combined) (≥0.05ng/mL). Specifically, passive and active smoking were defined as cotinine of 0.05–10 ng/mL, and ≥10ng/mL respectively.
Results
The prevalence of second-hand smoke exposure was 42.0% (95%CI, 36.7%-47.5%); while the prevalence of active smoking among teenagers was 9.0% (95%CI, 6.2%-12.5%). Vitamin D deficiency occurred at a frequency of 15.1% in children unexposed to tobacco smoke, 20.9% in children exposed to passive tobacco smoke, and 18.0% among actively smoking youth (p<0.001). Tobacco smoke exposure independently predicted vitamin D deficiency after controlling for age, sex, race, BMI, maternal education, and family socio-economic status (OR:1.50; 95%CI, 1.14–1.85, p = 0.002).
Conclusions: This analysis of a nationwide database reports that tobacco smoke exposure is an independent predictor of vitamin D deficiency in US children.
Title revision Nov 2019 caused the visitor count to reset.
There have actually been visitors to this page since it was originally made