Cardiovascular Disease and vitamin D – no proof yet
Optimal Vitamin D Supplementation Levels for Cardiovascular Disease Protection.
Dis Markers. 2015;2015:864370. doi: 10.1155/2015/864370. Epub 2015 Sep 8.
Lugg ST1, Howells PA1, Thickett DR1.
1School of Clinical and Experimental Medicine, College of Medical and Dental Sciences, Centre for Translational Inflammation Research (CTIR), University of Birmingham Laboratories, Queen Elizabeth Hospital Birmingham, Birmingham B15 2TH, UK.
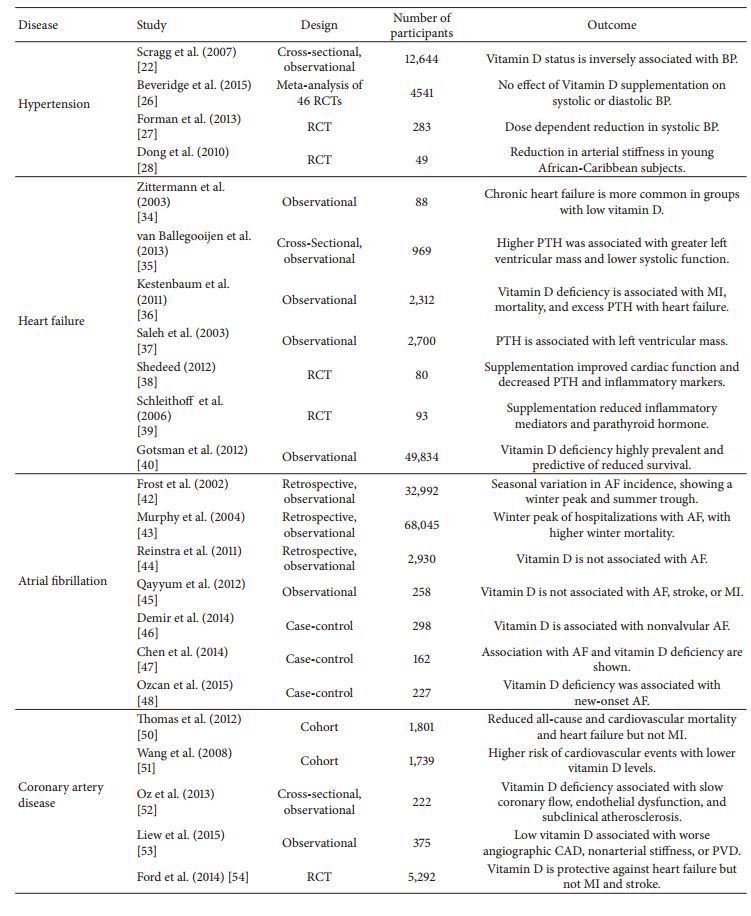
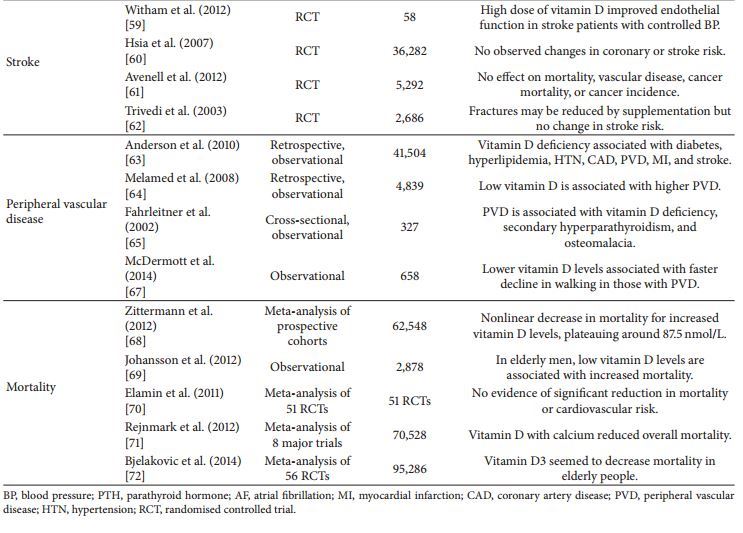
First described in relation to musculoskeletal disease, there is accumulating data to suggest that vitamin D may play an important role in cardiovascular disease (CVD). In this review we aim to provide an overview of the role of vitamin D status as both a marker of and potentially causative agent of hypertension, coronary artery disease, heart failure, atrial fibrillation, stroke, and peripheral vascular disease. The role of vitamin D levels as a disease marker for all-cause mortality is also discussed. We review the current knowledge gathered from experimental studies, observational studies, randomised controlled trials, and subsequent systematic reviews in order to suggest the optimal vitamin D level for CVD protection.
||Vitamin D status |nmol/L| ng/mL
Toxicity |>375 |>150
Optimal |100–150| 40–60
Sufficient |75–99 |30–39
Insufficient |50–74 |20–29
Deficient| <50 |<20||
Conclusions
There are weak signals of benefit of vitamin D supplementation
in heart failure, whilst studies have so far shown vitamin
D to be ineffective as an agent in lowering blood pressure and
thus it should not be used as an antihypertensive agent. In
CAD, AF, PVD, and stroke, although low vitamin D levels
are associated with disease occurrence, supplementation has
not yet been shown to be of benefit. Whether vitamin D is
a causal factor or convenient biomarker is not yet established
and maybe supplementation in cohorts of older adults may be
too late. Modest reductions in all-cause mortality by vitamin
D3 were demonstrated by meta-analysis [71], but the number
needed for benefit was around 150 and, due to attrition bias,
the reliability of the estimate was low.
On the other hand, vitamin D deficiency is very prevalent
and modest improvements might make substantial health
gains, with a low risk of adverse outcome. On the strength
of current evidence, supplementation for optimum cardiovascular
outcomes alone does not seem to be a justifiable
position, but, for overall health, following IOM [74] and
National Institute for Health and Care (NICE) guidance [80]
is the best effort to answer an underinvestigated question. A
number of areas, particularly heart failure, warrant controlled
trials look for robust evidence for a potentially cheap, low risk,
and effective treatment option
📄 Download the PDF from VitaminDWiki