Calcifediol (Calcidiol) might be a better form of Vitamin D for some people
Hypovitaminosis D: Is It Time to Consider the Use of Calcifediol?
Nutrients. 2019 May 6;11(5). pii: E1016. doi: 10.3390/nu11051016.
Cesareo R1, Falchetti A2, Attanasio R3, Tabacco G4, Naciu AM5, Palermo A6.
One company sells Calcifediol on Amazon as of Dec 2025
 click on image for details
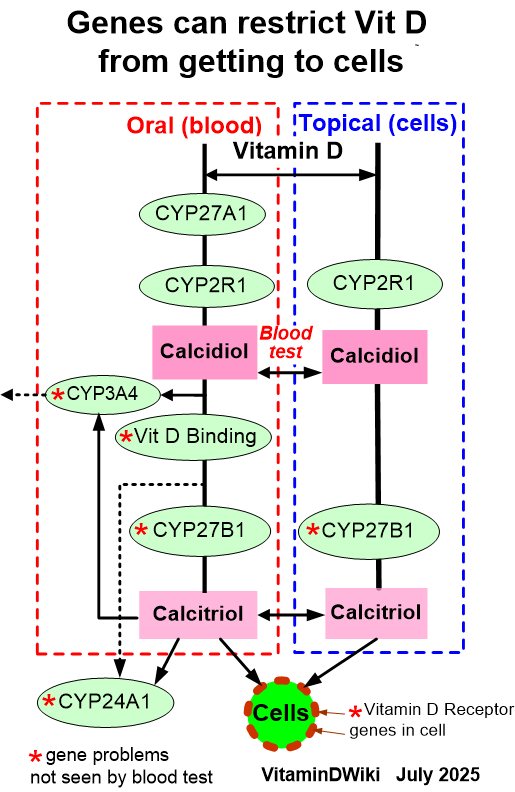
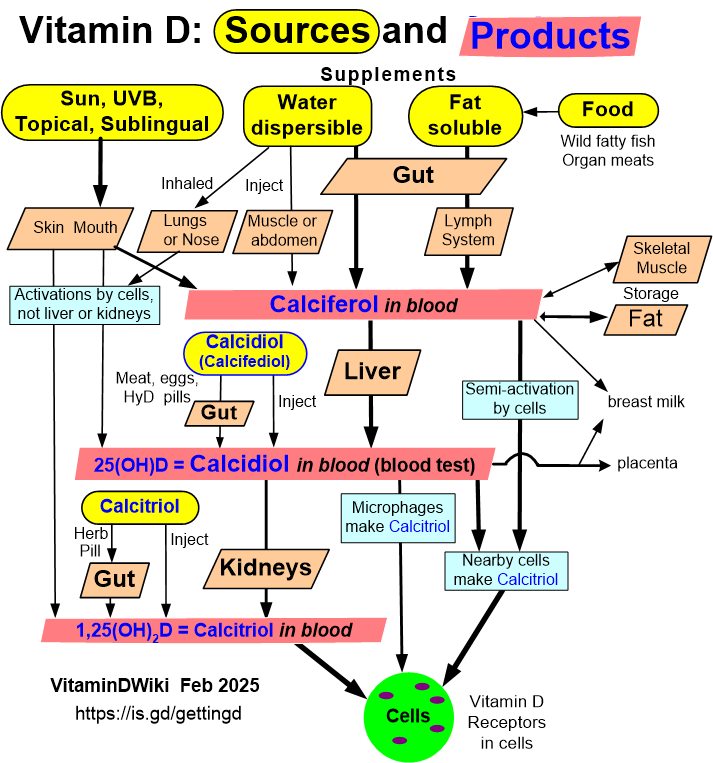
1. Getting Vitamin D into your blood and cells has the following chart
click on image for details
1. Getting Vitamin D into your blood and cells has the following chart
 Note: Apparently Calcidiol does not increase Vitamin D in BREAST Milk
Note: The word BREAST does not occur once in the PDF
---
1. Addtional Alternate ways of increasing Vitamin D levels for those with poor guts
* Nanoemulsion Vitamin D may be a substantially better form
* Sun/UV
* Injection
* Topical
* Inhaled
Note: Apparently Calcidiol does not increase Vitamin D in BREAST Milk
Note: The word BREAST does not occur once in the PDF
---
1. Addtional Alternate ways of increasing Vitamin D levels for those with poor guts
* Nanoemulsion Vitamin D may be a substantially better form
* Sun/UV
* Injection
* Topical
* Inhaled
📄 Download the PDF from VitaminDWiki
Hypovitaminosis D is becoming a notable health problem worldwide. A consensus exists among several different medical societies as to the need for adequate levels of vitamin D for bone and general health. The correct method by which to restore normal vitamin D levels is still a matter of debate. Although cholecalciferol remains the most commonly distributed form of vitamin D supplementation worldwide, several drugs with vitamin D activity are available for clinical use, and making the correct selection for the individual patient may be challenging. In this narrative review, we aim to contribute to the current knowledge base on the possible and appropriate use of calcifediol-the 25-alpha-hydroxylated metabolite-in relation to
its chemical characteristics,
its biological properties, and
its pathophysiological aspects.
Furthermore, we examine the trials that have aimed to evaluate the effect of calcifediol on the restoration of normal vitamin D levels.
Calcifediol is more soluble than cholecalciferol in organic solvents, due to its high polarity.
Good intestinal absorption and
high affinity for the vitamin-D-binding protein positively affect the bioavailability of calcifediol compared with cholecalciferol.
In particular,
- orally administered calcifediol shows a much shorter half-life than oral cholecalciferol.
Most findings suggest that oral calcifediol is about
three- to five-fold more powerful than oral cholecalciferol, and that it
has a higher rate of intestinal absorption.
Accordingly, calcifediol can be particularly useful in treating diseases associated with decreased intestinal absorption, as well as obesity (given its lower trapping in the adipose tissue ) and potentially neurological diseases treated with drugs that interfere with the hepatic cytochrome P-450 enzyme system, resulting in decreased synthesis of calcifediol. Up to now, there has not been enough clinical evidence for its use in the context of osteoporosis treatment.
From PDF
Conclusions: Time to Consider Calcifediol as an Adequate Supplement of Vitamin D?
Data from the literature are in accord in recommending vitamin D supplementation for all subjects at risk of vitamin D deficiency (Table 2), and the determination of vitamin D deficiency is cost-effective. 25(OH)D values of <20 ng/mL indicate a deficiency, but the requirement of supplementation is still controversial for values between 20 and 30 ng/mL [85]. The majority of the data on vitamin D supplementation in relation to human health almost exclusively involve cholecalciferol in registered clinical trials on anti-fracture drugs in subjects with reduced bone mass; the data highlight skeletal-related endpoints. All these trials have administered cholecalciferol supplementation, although sometimes with different dosages. Consequently, at the moment, robust, evidence-based data that unequivocally demonstrate the effects of the vitamin D hydroxylated metabolite on skeletal health are not available.
Table 2. Categories of patients that should be screened for vitamin D deficiency
Osteomalacia
Osteoporosis (particularly if bone-active drugs are to be used)
Older adults with a history of falls
Older adults with a history of non-traumatic fractures
Pregnant and lactating women
Obese children and adults
People with insufficient sun exposure
Malabsorption syndromes (congenital or acquired) and bariatric surgery
Chronic kidney disease
Hepatic failure
Cystic fibrosis
Hyperparathyroidism
People taking drugs that interfere with vitamin D metabolism
- (antiseizure medications, glucocorticoids, AIDS medications, antifungals, cholestyramine)
Granulomatous disorders and some lymphomas
In general, in subjects with hypovitaminosis D, oral calcifediol supplementation is more powerful for increasing serum 25(OH)D concentrations than cholecalciferol. In particular, the calculated relative potency of calcifediol versus cholecalciferol varied between 1.7 and 8 , depending on the doses, different pharmacokinetics, and basal 25(OH)D serum levels [6]. A formula has been proposed for calculating the expected increase in circulating 25(OH)D levels when vitamin D is supplemented, which considers age, the baseline 25(OH)D status, and body weight [106]. With this approach, much higher doses of vitamin D3 would be required to realize the same increase in serum 25(OH)D concentration as that observed with calcifediol [107]. In patients affected by hypovitaminosis D without reduced bone mass, calcifediol can be taken instead of cholecalciferol, because it is better able to increase circulating 25(OH)D levels without the need to use micro- or macro-boli.
To summarize, compared with cholecalciferol, calcifediol
is absorbed the best,
has a different volume of distribution,
is independent from hepatic 25-hydroxylase, and
produces a more rapid increase in circulating levels of 25(OH)D [6,62].
In particular, calcifediol is a more polar and soluble metabolite that may display smaller volumes of distribution, and less trapping by the adipose tissue [62]. Consequently, these aspects affect both its intestinal absorption and circulating DBP transport, as well as the whole body distribution of its orally administered metabolite, displaying a much shorter half-life (approximately 10-13 days) than the parental cholecalciferol [16,58,108-110]. The use of calcifediol might be more cost-effective in obese patients and in those with malabsorption syndromes. Its use may be beneficial in patients taking drugs that interfere with the hepatic cytochrome P-450 enzyme system, particularly corticosteroid drugs or anticonvulsants. Thus, at least in these specific conditions, calcifediol can be used as an alternative to cholecalciferol [111] and, assuming the above-described higher pharmacologic activity of oral calcifediol relative to oral cholecalciferol [6], the cost per IU of calcifediol could be about six time lower than that of cholecalciferol (according to the market prices in Italy in 2019) [112,113], although such a direct comparison between the costs of these different molecules cannot lead to an accurate and adequate proposal.
Quesada-Gomez JM and colleague suggested "oral calcifediol as a valid and favorable alternative for the prevention or treatment of osteoporosis" [6]. Instead, we are strongly convinced that further studies are needed to investigate the efficacy and safety of calcifediol in the clinical setting of bone