Risk of COVID not reduced by 3,200 IU of vitamin D during 6 months (no surprise) – RCT
Vitamin D Supplements for Prevention of Covid-19 or other Acute Respiratory Infections: a Phase 3 Randomized Controlled Trial (CORONAVIT)
PrePrint March 2022, doi: https://doi.org/10.1101/2022.03.22.22271707
Jolliffe, Hayley Holt, Matthew Greenig, Mohammad Talaei, Natalia Perdek, Paul Pfeffer, Sheena Maltby, Jane Symons, Nicola Barlow, Alexa Normandale, Rajvinder Garcha, Alex Richter, Sian Faustini, Christopher Orton, David Ford, Ronan Lyons, Gwyneth Davies, Frank Kee, Christopher Griffiths, John Norrie, Aziz Sheikh, Seif Shaheen, Clare Relton, Adrian Martineau
BACKGROUND: Vitamin D metabolites support innate immune responses to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and other respiratory pathogens. Randomized controlled trials of vitamin D to prevent coronavirus disease 2019 (Covid-19) have not yet reported.
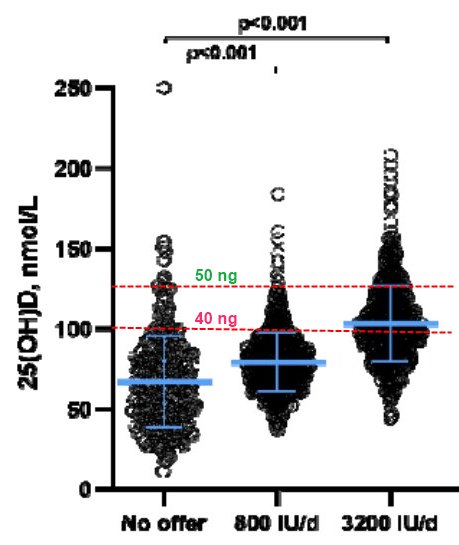
METHODS: We randomly assigned 6200 U.K. adults to receive an offer of a postal finger-prick 25-hydroxyvitamin D (25[OH]D) test with provision of a 6-month supply of higher-dose vitamin D ( 3200 IU/d , n=1550) or lower-dose vitamin D (800 IU/d, n=1550) to those with blood 25(OH)D concentration <75 nmol/L, vs. no offer of testing or supplementation (n=3100). The primary outcome was the proportion of participants experiencing at least one swab test- or doctor-confirmed acute respiratory infection (ARI) of any cause at six months. Secondary outcomes included incidence of swab test-confirmed Covid-19.
RESULTS: Of 3100 participants offered testing, 2958 (95.4%) accepted, and 2690 (86.8%) had 25(OH)D <75 nmol/L and were sent vitamin D supplements (1356 higher-dose, 1334 lower-dose). 76 (5.0%) vs. 87 (5.7%) vs. 136 (4.6%) participants in higher-dose vs. lower-dose vs. no-offer groups experienced at least one ARI of any cause (odds ratio [OR] for higher-dose vs. no-offer 1.09, 95% CI 0.82-1.46; lower-dose vs. no-offer 1.26, 0.96-1.66). 45 (3.0%) vs. 55 (3.6%) vs. 78 (2.6%) participants in higher-dose vs. lower-dose vs. no-offer groups developed Covid-19 (OR for higher-dose vs. no-offer 1.13, 0.78-1.63; lower-dose vs. no-offer 1.39, 0.98-1.97).
CONCLUSIONS: Among adults with a high baseline prevalence of vitamin D insufficiency, implementation of a test-and-treat approach to vitamin D replacement did not reduce risk of all-cause ARI or Covid-19.
Clinical Trial NCT04579640
📄 Download preprint PDF from VitaminDWiki
📄 Download final PDF from VitaminDWiki
Major problem - did not wait for Vitamin D levels to plateau before gettng infection data
The trial appears to have started collecting data just 1 month after starting Vitamin D dosing
At that point, probably <10% had levels >40 ng. (thus very unlikely to have any benefit)
Also, even at the end of the 6 months about half of the participants still had levels <40 ng
VitaminDWiki - 36 studies have found that 5,000 IU gets only about half to >40 ng
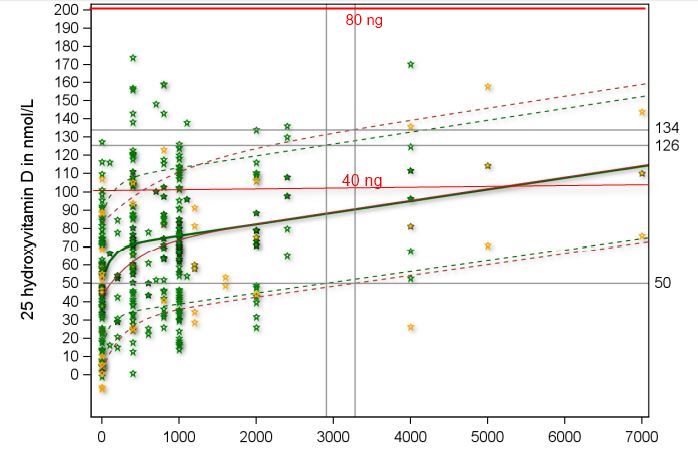
Appears that would need >12,000 IU to get most >50 ng
Many studies are finding at >50 ng level of vitamin D is needed to fight COVID
COVID fought by 50 ng of Vitamin D
{include}
VitaminDWiki – Is 50 ng the level needed?
Is 50 ng of vitamin D too high, just right, or not enough contains the following
{include}
VitaminDWiki – COVID-19 treated by Vitamin D - studies, reports, videos
{include}
VitaminDWiki – Loading (not daily) doses quickly raise Vitamin D levels and fight Viruses
This list is automatically updated
{category}