Overview Thyroid and Vitamin D
See VitaminDWiki
PTH reduced 3.5 pmol by vitamin D intervention which added 22 ng – meta-analysis June 2014
Autoimmune Thyroid Disease 3X more likely if low vitamin D – meta-analysis April 2015
PTH does not plateau with increasing vitamin D, but does decrease with patient age – Aug 2012
Vitamin D and Iodine are similar, and both are deficient and important to health
See also Web
Essential Guide to Understanding and Optimizing Thyroid Health Mercola] Nov 2024
- Vitamin D is NOT mentoned 📄 transcript
-
- Overall, our review suggested that the current evidence to support any protective or hazardous effect of vitamin or mineral supplements on thyroid cancer development is inconclusive and additional studies addressing previous limitations are necessary to elucidate this possible association.
- In particular, reverse causality is of major concern and should be addressed by prospective studies with large and representative samples.
Why Do I Still Have Thyroid Symptoms Weston A Price
Garry Shandling (commedian) died of hyperparathyroidism March 2016
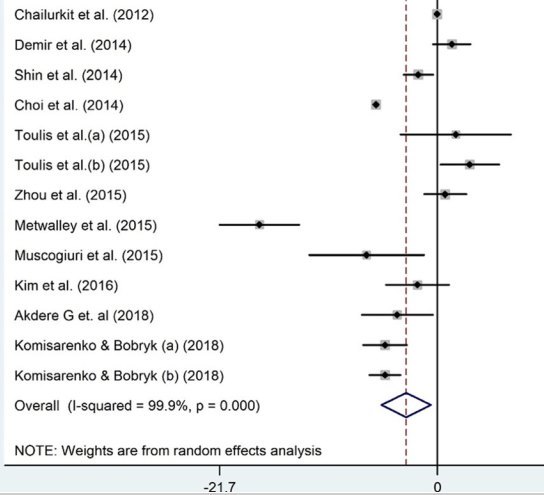
Thyroid disorders are associated with low vitamin D – meta-analysis Aug 2021
Vitamin D and thyroid disorders: a systematic review and Meta-analysis of observational studies
BMC Endocr Disord. 2021 Aug 21;21(1):171. doi: 10.1186/s12902-021-00831-5.
Sorour Taheriniya 1, Arman Arab 2, Amir Hadi 3, Abdulmannan Fadel 4, Gholamreza Askari 5
Background: The contribution of vitamin D to thyroid disorders has received paramount attention; however, results are mixed. Hence, we designed a systematic review and meta-analysis to obtain a definitive conclusion.
Methods: The search included PubMed, ISI Web of Science, Scopus, and Google Scholar databases up to March 2021 to collect available papers reporting the relationship between serum levels of vitamin D and thyroid disorders. The pooled effect was reported as weighted mean difference (WMD) and 95% confidence interval (CI).
Results: Out of 6123 datasets, 42 were eligible to get into this systematic review and meta-analysis.
Serum vitamin D was markedly lower in
| autoimmune thyroid diseases (AITD) | (WMD - 3.1 ng/dl; 95% CI, - 5.57 to - 0.66; P = 0.013; I2 = 99.9%), |
| Hashimoto's thyroiditis (HT) | (WMD - 6.05 ng/dl; 95% CI, - 8.35 to - 3.75; P < 0.001; I2 = 91.0%) and |
| hypothyroidism patients | (WMD - 13.43 ng/dl; 95% CI, - 26.04 to - 0.81; P = 0.03; I2 = 99.5%), |
but not in subjects with Graves' disease (GD) (WMD - 4.14 ng/dl; 95% CI, - 8.46 to 0.17; P = 0.06; I2 = 97.5%).
Conclusions: Our findings suggested lower vitamin D levels in patients with hypothyroidism, AITD, and HT compared to healthy subjects. However, the link between serum vitamin D and GD was only significant among subjects ≥40 years old.
autoimmune thyroid diseases
📄 Download the PDF from VitaminDWiki
References
Skaaby T, Husemoen LLN, Thuesen BH, Linneberg A. Prospective population-based study of the association between vitamin D status and incidence of autoimmune disease. Endocrine. 2015;50(1):231–8. https://doi.org/10.1007/s12020-015-0547-4 . - DOI - PubMed
Vatandost S, Jahani M, Afshari A, Amiri MR, Heidarimoghadam R, Mohammadi Y. Prevalence of vitamin D deficiency in Iran: a systematic review and meta-analysis. Nutr Health. 2018;24(4):269–78. https://doi.org/10.1177/0260106018802968 . - DOI - PubMed
Hassan-Smith ZK, Hewison M, Gittoes NJ. Effect of vitamin D deficiency in developed countries. Br Med Bull. 2017;122(1):79–89. https://doi.org/10.1093/bmb/ldx005 . - DOI - PubMed
Kelishadi R, Qorbani M, Motlagh ME, Heshmat R, Poursafa P, Bahreynian M. Prevalence of vitamin D deficiency according to climate conditions among a nationally representative sample of Iranian adolescents: the CASPIAN-III study. Int J Pediatr. 2016;4(6):1903–10.
Cashman KD, Dowling KG, Škrabáková Z, Gonzalez-Gross M, Valtueña J, De Henauw S, et al. Vitamin D deficiency in Europe: pandemic? Am J Clin Nutr. 2016;103(4):1033–44. https://doi.org/10.3945/ajcn.115.120873 . - DOI - PubMed - PMC
LeFevre ML. Screening for vitamin D deficiency in adults: US preventive services task force recommendation statement. Ann Intern Med. 2015;162(2):133–40. https://doi.org/10.7326/M14-2450 . - DOI - PubMed
Arabi A, El Rassi R, Fuleihan GE-H. Hypovitaminosis D in developing countries—prevalence, risk factors and outcomes. Nat Rev Endocrinol. 2010;6(10):550–61. https://doi.org/10.1038/nrendo.2010.146 . - DOI - PubMed
Pludowski P, Holick MF, Pilz S, Wagner CL, Hollis BW, Grant WB, et al. Vitamin D effects on musculoskeletal health, immunity, autoimmunity, cardiovascular disease, cancer, fertility, pregnancy, dementia and mortality—a review of recent evidence. Autoimmun Rev. 2013;12(10):976–89. https://doi.org/10.1016/j.autrev.2013.02.004 . - DOI - PubMed
Spiro A, Buttriss J. Vitamin D: an overview of vitamin D status and intake in E urope. Nutr Bull. 2014;39(4):322–50. https://doi.org/10.1111/nbu.12108 . - DOI - PubMed - PMC
Hossein-nezhad A, Holick MF: Vitamin D for health: a global perspective. In: Mayo clinic proceedings: 2013: Elsevier; 2013: 720–755.
Ławnicka H, Galant-Gdula A, Motylewska E, Komorowski J, Świętosławski J, Stępień H. Estimation of vitamin D status in patients with secondary and primary hypothyroidism of different etiology. Neuroendocrinol Lett. 2017;38(8):565-74.
Feng M, Li H, Chen SF, Li WF, Zhang FB. Polymorphisms in the vitamin D receptor gene and risk of autoimmune thyroid diseases: a meta-analysis. Endocrine. 2013;43(2):318–26. https://doi.org/10.1007/s12020-012-9812-y . - DOI - PubMed
Maenhaut C, Christophe D, Vassart G, Dumont J, Roger P, Opitz R: Ontogeny, anatomy, metabolism and physiology of the thyroid. In: Endotext [Internet]. edn.: MDText. com, Inc.; 2015.
Degroot LJ, Quintans J. The causes of autoimmune thyroid disease. Endocr Rev. 1989;10(4):537–62. https://doi.org/10.1210/edrv-10-4-537 . - DOI - PubMed
Nettore IC, Albano L, Ungaro P, Colao A, Macchia PE. Sunshine vitamin and thyroid. Reviews in Endocrine and Metabolic Disorders. 2017;18(3):347–54. https://doi.org/10.1007/s11154-017-9406-3 . - DOI - PubMed
Goswami R, Marwaha RK, Gupta N, Tandon N, Sreenivas V, Tomar N, et al. Prevalence of vitamin D deficiency and its relationship with thyroid autoimmunity in Asian Indians: a community-based survey. Br J Nutr. 2009;102(3):382–6. https://doi.org/10.1017/S0007114509220824 . - DOI - PubMed
Musa IR, Gasim GI, Khan S, Ibrahim IA, Abo-alazm H, Adam I. No association between 25 (OH) vitamin D level and hypothyroidism among females. Open access Macedonian journal of medical sciences. 2017;5(2):126–30. https://doi.org/10.3889/oamjms.2017.029 . - DOI - PubMed - PMC
Effraimidis G, Badenhoop K, Tijssen JG, Wiersinga WM. Vitamin D deficiency is not associated with early stages of thyroid autoimmunity. Eur J Endocrinol. 2012;167(1):43–8. https://doi.org/10.1530/EJE-12-0048 . - DOI - PubMed
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. https://doi.org/10.1186/2046-4053-4-1 . - DOI - PubMed - PMC
Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Ottawa Hospital Research Institute; 2011.
Uhland AM, Kwiecinski GG, DeLuca HF. Normalization of serum calcium restores fertility in vitamin D-deficient male rats. J Nutr. 1992;122(6):1338–44. https://doi.org/10.1093/jn/122.6.1338 . - DOI - PubMed
Von Hippel PT. Mean, median, and skew: Correcting a textbook rule. J Stat Educ. 2005;13(2):1-13.
Green S, Higgins J: Cochrane handbook for systematic reviews of interventions. In: Version; 2005.
Yang CH, Albietz J, Harkin DG, Kimlin MG, Schmid KL. Impact of oral vitamin D supplementation on the ocular surface in people with dry eye and/or low serum vitamin D. Contact lens & anterior eye : the journal of the British Contact Lens Association. 2018;41(1):69–76. https://doi.org/10.1016/j.clae.2017.09.007 . - DOI
Bouillon R, Muls E, De Moor P. Influence of thyroid function on the serum concentration of 1,25-dihydroxyvitamin D3. J Clin Endocrinol Metab. 1980;51(4):793–7. https://doi.org/10.1210/jcem-51-4-793 . - DOI - PubMed
Unal AD, Tarcin O, Parildar H, Cigerli O, Eroglu H, Demirag NG. Vitamin D deficiency is related to thyroid antibodies in autoimmune thyroiditis. Central European Journal of Immunology. 2014;39(4):493–7. https://doi.org/10.5114/ceji.2014.47735 . - DOI - PubMed - PMC
Ma J, Wu D, Li C, Fan C, Chao N, Liu J, et al. Lower serum 25-Hydroxyvitamin D level is associated with 3 types of autoimmune thyroid diseases. Medicine. 2015;94(39):e1639. https://doi.org/10.1097/MD.0000000000001639 . - DOI - PubMed - PMC
Ke W, Sun T, Zhang Y, He L, Wu Q, Liu J, et al. 25-Hydroxyvitamin D serum level in Hashimoto's thyroiditis, but not Graves' disease is relatively deficient. Endocr J. 2017;64(6):581–7. https://doi.org/10.1507/endocrj.EJ16-0547 . - DOI - PubMed
Fawzy E, MD, Mohamed SA-S, Shebl M, El-Rabat AM. Hypovitaminosis d in autoimmune hypothyroidism. Journal Of American Science. 2013;9(11):60-5.
Toulis K, Tsekmekidou X, Potolidis E, Didangelos T, Gotzamani-Psarrakou A, Zebekakis P, et al. Thyroid autoimmunity in the context of type 2 diabetes mellitus: implications for vitamin D. Int J Endocrinol. 2015;2015:1–5. https://doi.org/10.1155/2015/710363 . - DOI
Komisarenko YI, Bobryk MI. Vitamin D deficiency and immune disorders in combined endocrine pathology. Front Endocrinol. 2018;9. https://doi.org/10.3389/fendo.2018.00600 .
Mackawy AMH, Al-Ayed BM, Al-Rashidi BM. Vitamin D deficiency and its association with thyroid disease. Int J Health Sci. 2013;7(3):267–75. https://doi.org/10.12816/0006054 . - DOI
Mirhosseini N, Brunel L, Muscogiuri G, Kimball S. Physiological serum 25-hydroxyvitamin D concentrations are associated with improved thyroid function—observations from a community-based program. Endocrine. 2017;58(3):563–73. https://doi.org/10.1007/s12020-017-1450-y . - DOI - PubMed - PMC
Ucar F, Akyol S, Ozturk G, Ginis Z, Erden G, Taslipinara MY, et al. Evaluation of serum vitamin D levels in elderly patients with subclinical hypothyroidism. J Exper Clin Med (Turkey). 2014;31(2):77–80. https://doi.org/10.5835/jecm.omu.31.02.003 . - DOI
Aljohani NJ, Al-Daghri NM, Al-Attas OS, Alokail MS, Alkhrafy KM, Al-Othman A, et al. Differences and associations of metabolic and vitamin D status among patients with and without sub-clinical hypothyroid dysfunction. BMC Endocr Disord. 2013;13(1). https://doi.org/10.1186/1472-6823-13-31 .
Bozkurt NC, Karbek B, Ucan B, Sahin M, Cakal E, Ozbek M, et al. THE ASSOCIATION BETWEEN SEVERITY OF VITAMIN D DEFICIENCY AND HASHIMOTO'S THYROIDITIS. Endocr Pract. 2013;19(3):479–84. https://doi.org/10.4158/EP12376.OR . - DOI - PubMed
Camurdan OM, Doger E, Bideci A, Celik N, Cinaz P. Vitamin D status in children with Hashimoto thyroiditis. Journal of pediatric endocrinology & metabolism : JPEM. 2012;25(5–6):467–70.
Ławnicka H, Galant-Gdula A, Motylewska E, Komorowski J, Świȩtosławski J, Stȩpień H. Estimation of vitamin D status in patients with secondary and primary hypothyroidism of different etiology. Neuroendocrinol Lett. 2017;38(8):565–74.
Evliyaoglu O, Acar M, Ozcabi B, Erginoz E, Bucak F, Ercan O, et al. Vitamin D deficiency and Hashimoto's thyroiditis in children and adolescents: a critical vitamin D level for this association? Journal of clinical research in pediatric endocrinology. 2015;7(2):128–33. https://doi.org/10.4274/jcrpe.2011 . - DOI - PubMed - PMC
Giovinazzo S, Vicchio TM, Certo R, Alibrandi A, Palmieri O, Campenni A, et al. Vitamin D receptor gene polymorphisms/haplotypes and serum 25(OH)D3 levels in Hashimoto's thyroiditis. Endocrine. 2016;55(2):599–606. https://doi.org/10.1007/s12020-016-0942-5 . - DOI - PubMed
Maciejewski A, Wojcicka M, Roszak M, Losy J, Lacka K. Assessment of vitamin D level in autoimmune thyroiditis patients and a control Group in the Polish Population. Adv Clin Exp Med. 2015;24(5):801–6. https://doi.org/10.17219/acem/29183 . - DOI - PubMed
Nalbant A, Gokosmanoglu F, Cinemre H, Varim C, Kaya T, Ergenc H. The relation between serum vitamin D levels and Hashimoto thyroiditis in women. Kuwait Med J. 2017;49(3):223–6.
Sönmezgöz E, Ozer S, Yilmaz R, Önder Y, Bütün I, Bilge S. Hypovitaminosis d in children with hashimoto’s thyroiditis. Revista Medica de Chile. 2016;144(5):611–6. https://doi.org/10.4067/S0034-98872016000500009 . - DOI - PubMed
Botelho IMB, Moura Neto A, Silva CA, Tambascia MA, Alegre SM, Zantut-Wittmann DE. Vitamin D in Hashimoto's thyroiditis and its relationship with thyroid function and inflammatory status. Endocr J. 2018;65(10):1029–37. https://doi.org/10.1507/endocrj.EJ18-0166 . - DOI - PubMed
Jyotsna VP, Sahoo A, Ksh SA, Sreenivas V, Gupta N. Bone mineral density in patients of graves disease pre- & post-treatment in a predominantly vitamin D deficient population. Indian J Med Res. 2012;135(1):36–41. https://doi.org/10.4103/0971-5916.93422 . - DOI - PubMed - PMC
Planck T, Shahida B, Malm J, Manjer J. Vitamin D in graves disease: levels, correlation with laboratory and clinical parameters, and genetics. Eur Thyroid J. 2017;7(1):27–33. https://doi.org/10.1159/000484521 . - DOI - PubMed - PMC
Yasuda T, Okamoto Y, Hamada N, Miyashita K, Takahara M, Sakamoto F, et al. Serum vitamin D levels are decreased and associated with thyroid volume in female patients with newly onset Graves' disease. Endocrine. 2012;42(3):739–41. https://doi.org/10.1007/s12020-012-9679-y . - DOI - PubMed - PMC
Demir K, Keskin M, Kor Y, Karaoglan M, Bulbul OG. Autoimmune thyroiditis in children and adolescents with type 1 diabetes mellitus is associated with elevated IgG4 but not with low vitamin D. Hormones Int J Endocrinol Metab. 2014;13(3):361–8.
Akdere G, Efe B, Sisman P, Yorulmaz G. The relationship between vitamin D level and organ-specific autoimmune disorders in newly diagnosed type I diabetes mellitus. Bratislava Med J Bratislavske Lekarske Listy. 2018;119(9):544–9. https://doi.org/10.4149/BLL2018098 . - DOI
Metwalley KA, Farghaly HS, Sherief T, Hussein A. Vitamin D status in children and adolescents with autoimmune thyroiditis. J Endocrinol Investig. 2015;39(7):793–7. - DOI
Zhang H, Liang L, Xie Z. Low vitamin D status is associated with increased thyrotropin-receptor antibody titer in graves disease. Endocr Pract. 2014;21(3):258–63. - DOI
Kmieć P, Minkiewicz I, Rola R, Sworczak K, Żmijewski MA, Kowalski K. Vitamin D status including 3-epi-25 (OH) D3 among adult patients with thyroid disorders during summer months. Endokrynologia Polska. 2018;69(6):653–60. https://doi.org/10.5603/EP.a2018.0065 . - DOI - PubMed
Chailurkit LO, Aekplakorn W, Ongphiphadhanakul B. High vitamin D status in younger individuals is associated with low circulating thyrotropin. Thyroid. 2012;23(1):25–30. https://doi.org/10.1089/thy.2012.0001 . - DOI - PubMed
Shin DY, Kim KJ, Kim D, Hwang S, Lee EJ. Low serum vitamin D is associated with anti-thyroid peroxidase antibody in autoimmune thyroiditis. Yonsei Med J. 2014;55(2):476–81. https://doi.org/10.3349/ymj.2014.55.2.476 . - DOI - PubMed - PMC
Choi YM, Kim WG, Kim TY, Bae SJ, Kim HK, Jang EK, et al. Low levels of serum vitamin D3 are associated with autoimmune thyroid disease in pre-menopausal women. Thyroid : official journal of the American Thyroid Association. 2014;24(4):655–61. https://doi.org/10.1089/thy.2013.0460 . - DOI
Zhou P, Cai JN, Markowitz M. Absence of a relationship between thyroid hormones and vitamin D levels. J Pediatr Endocrinol Metab. 2015;29(6):703–7.
Muscogiuri G, Palomba S, Caggiano M, Tafuri D, Colao A, Orio F. Low 25 (OH) vitamin D levels are associated with autoimmune thyroid disease in polycystic ovary syndrome. Endocrine. 2015;53(2):538–42. https://doi.org/10.1007/s12020-015-0745-0 . - DOI - PubMed
Kim D. Low vitamin D status is associated with hypothyroid Hashimoto's thyroiditis. Hormones Int J Endocrinol Metab. 2016;15(3):385–93.
Maciejewski A, Wojcicka M, Roszak M, Losy J, Lacka K. Assessment of vitamin D level in autoimmune thyroiditis patients and a control Group in the Polish Population. Advances in clinical and experimental medicine : official organ Wroclaw Medical University. 2015;24(5):801–6. https://doi.org/10.17219/acem/29183 . - DOI
Esmat Fawzy M, Mohamed SA-S, Shebl M, El-Rabat AM. Hypovitaminosis d in autoimmune hypothyroidism. Journal Of American Science. 2013;9(11):60-5.
Kmiec P, Minkiewicz I, Rola R, Sworczak K, Zmijewski MA, Kowalski K. Vitamin D status including 3-epi-25(OH)D-3 among adult patients with thyroid disorders during summer months. Endokrynologia Polska. 2018;69(6):653–60. https://doi.org/10.5603/EP.a2018.0065 . - DOI - PubMed
Muscogiuri G, Tirabassi G, Bizzaro G, Orio F, Paschou SA, Vryonidou A, et al. Vitamin D and thyroid disease: to D or not to D? Eur J Clin Nutr. 2015;69(3):291–6. https://doi.org/10.1038/ejcn.2014.265 . - DOI - PubMed
Snellman G, Melhus H, Gedeborg R, Byberg L, Berglund L, Wernroth L, et al. Determining vitamin D status: a comparison between commercially available assays. PLoS One. 2010;5(7):e11555. https://doi.org/10.1371/journal.pone.0011555 . - DOI - PubMed - PMC
Diffey B. Modelling the seasonal variation of vitamin D due to sun exposure. Br J Dermatol. 2010;162(6):1342–8. https://doi.org/10.1111/j.1365-2133.2010.09697.x . - DOI - PubMed
Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF. Decreased bioavailability of vitamin D in obesity. Am J Clin Nutr. 2000;72(3):690–3. https://doi.org/10.1093/ajcn/72.3.690 . - DOI - PubMed
Wang X, Cheng W, Ma Y, Zhu J. Vitamin D receptor gene FokI but not TaqI, ApaI, BsmI polymorphism is associated with Hashimoto’s thyroiditis: a meta-analysis. Sci Rep. 2017;7(1):1–11. - DOI
Yazici D, Yavuz D, Tarcin O, Sancak S, Deyneli O, Akalin S. Vitamin D receptor gene ApaI, TaqI, FokI and BsmI polymorphisms in a group of Turkish patients with Hashimoto's thyroiditis. Minerva Endocrinol. 2013;38(2):195–201. - PubMed
Altieri B, Muscogiuri G, Barrea L, Mathieu C, Vallone CV, Mascitelli L, et al. Does vitamin D play a role in autoimmune endocrine disorders? A proof of concept. Rev Endocr Metab Disord. 2017;18(3):335–46. https://doi.org/10.1007/s11154-016-9405-9 . - DOI - PubMed
Aranow C. Vitamin D and the immune system. J Investig Med. 2011;59(6):881–6. https://doi.org/10.2310/JIM.0b013e31821b8755 . - DOI - PubMed - PMC
Wang X, Zynat J, Guo Y, Osiman R, Tuhuti A, Zhao H, et al. Low serum vitamin D is associated with anti-thyroid-globulin antibody in female individuals. Int J Endocrinol. 2015;2015:285290. - PubMed - PMC
Zhang Q, Sun M, Wang Z, Fu Q, Shi Y, Yang F, et al. Relationship between serum 25-hydroxy vitamin D and thyroid autoimmunity among middle-aged and elderly individuals. Acta Univ Med Nanjing (Nat Sci). 2014;34:486–9.
Łacka K, Maciejewski A. Vitamin D in the etiopathogenesis of autoimmune thyroiditis. Polski Merkuriusz Lekarski. 2013;34(203):281–5. - PubMed
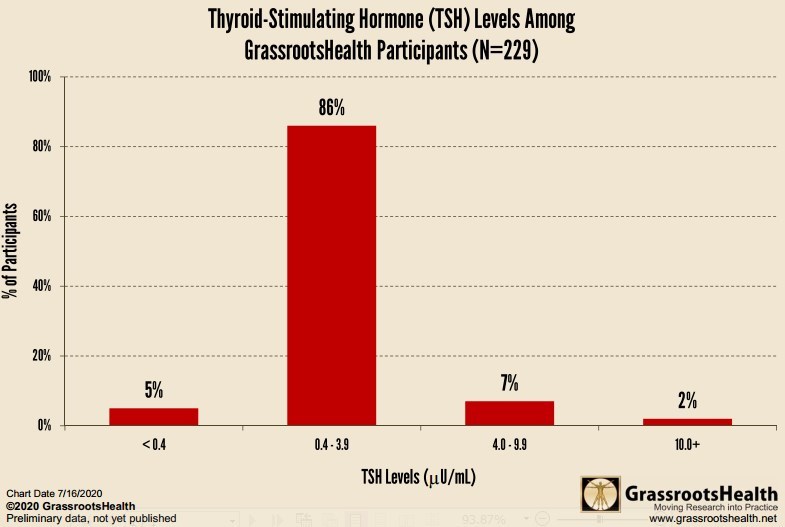
Thyroid-Stimulating Hormone at Grassroots Health - July 2020
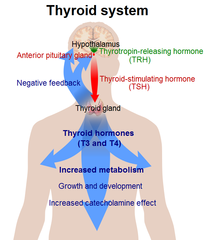
Thyroid-stimulating hormone (TSH) is a hormone produced by the pituitary gland that stimulates the production of hormones from the thyroid that are essential to many bodily functions such as metabolism, brain development, bone health, muscle control, heart rate, and body temperature.
Thyroid dysfunction is under-diagnosed with some population studies indicating that up to 10% of Americans may have thyroid dysfunction. A TSH test can indicate whether your thyroid gland is working normally, or if it’s overactive (hyperthyroidism) or underactive (hypothyroidism). An overactive thyroid gland can produce symptoms such as irritability, diarrhea, heart palpitations, heat sensitivity, and insomnia while an underactive thyroid gland can produce fatigue, unexplained weight gain, infertility, and mood swings. A TSH test can detect thyroid dysfunction before you have any symptoms.
The normal TSH range depends on a person’s age and pregnancy status, with levels tending to be higher as a person gets older and lower during pregnancy. According to the American Thyroid Association, doctors generally consider levels between 0.4 and 4.0 µU/mL to be within the normal range with levels between 0.0 and 0.4 µU/mL indicating hyperthyroidism, levels between 4.0 and 10.0 µU/mL indicating mild hypothyroidism, and levels 10 µU/mL or higher indicating hypothyroidism. However, some experts consider normal levels to be between 0.5 and 2.0-2.5 µU/mL.
Additional tests may be recommended if TSH levels are out of range to give a more definitive diagnosis of thyroid disease or dysfunction. The treatment and diagnosis must be undertaken with a medical doctor or other primary health care provider.
What are the TSH levels among GrassrootsHealth Participants?
GrassrootsHealth offers a TSH dried blood spot test. Among the 229 participants who have tested their TSH levels, the average level was 1.5 µU/mL. As you can see from the chart below, 86% of these participants have levels in the normal range, 5% have levels in the range indicating possible hyperthyroidism, 7% have levels in the range indicating possible mild hypothyroidism, and 2% have levels indicating possible hypothyroidism.
Calcium, Parathyroid Hormone, and Vitamin D in Patients with Primary Hyperparathyroidism: Normograms Developed from 10,000 Cases. - 2010
Endocr Pract. 2010 Dec 6:1-26.
Norman J, Goodman A, Politz D.
Norman Parathyroid Center, Tampa, Florida.
Objective: To define more clearly the typical and atypical biochemical profiles of patients with surgically proven primary hyperparathyroidism.
Methods: A single-center, prospectively conducted study of serum calcium, parathyroid hormone, and Vitamin D in 10,000 consecutive patients over a 7 year period with surgically proven PHPT. Over 210,000 calcium, PTH, and vitamin D values were evaluated.
Results: Both calcium and PTH levels demonstrate a Gaussian distribution with the average calcium being 10.9±0.6 mg/dl and the average PTH being 105.8±48 pg/ml. The average highest calcium and PTH was 11.4±0.7 mg/dl and 115.3±50 pg/ml, respectively. At least one calcium level of 11.0 mg/dl is seen in 87% of patients, but only 21% had one or more calcium levels above 11.5 mg/dl. Only 7% had a single serum calcium level reaching 12.0 mg/dl. Normocalcemic HPT was seen in 2.5% of patients who had identical findings at surgery. An average PTH less than 65 pg/ml was seen in 16.5% with 10.5% having zero high PTH values. The average vitamin D-25 was 22.4±9 ng/ml, with levels decreasing as calcium levels increased (p<0.001); 36% had vitamin D-25 levels below 20ng/ml.
Conclusion: Patients with PHPT present with a number of distinct biochemical profiles, but as a group present with a near-normal Gaussian distribution of both calcium and PTH. Either serum calcium or PTH remained normal in 13% of patients yet the findings at surgery are similar to those with elevated calcium or PTH. Low vitamin D is an expected finding in patients with PHPT, decreasing as serum calcium levels increased. PMID: 21134884
[tiki-download_file.php?fileId=1651]
Example normogram
High vitamin D is associated with low TSH = Thyroid-stimulating hormone = Thyrotropin - 2012
High Vitamin D Status in Younger Individuals is Associated with Low Circulating Thyrotropin
Thyroid. 2012 Aug 30.
Chailurkit LO, Aekplakorn W, Ongphiphadhanakul B.
Ramathibodi Hospital, Medicine, Bangkok, Thailand; ralcl@mahidol.ac.th.
Background: Vitamin D is an immunomodulator and may affect autoimmune thyroid diseases. Vitamin D has also been shown to influence thyrocytes directly by attenuating the thyrotropin (TSH) stimulated iodide uptake and cell growth. However, it is unclear how vitamin D status is related to TSH at the population level. The goal of the present study was to investigate the relationship between vitamin D status and TSH levels according to thyroid autoantibodies in a population-based health survey in Thailand.
Methods: A total of 2,582 adults, aged 15-98 years, were randomly selected according to geographical region from the Thailand 4th National Health Examination Survey sample. Serum levels of 25-hydroxyvitamin D (25(OH)D), TSH, thyroid peroxidase antibody (TPOAb) and thyroglobulin antibody (TgAb) were measured in all subjects.
Results: The mean age was 55.0 ± 0.4 (SE) years. Fifty percent of the subjects were males. In subjects positive for serum TgAb, serum TSH levels were higher whereas total serum 25(OH)D levels were lower. In addition, the prevalence of vitamin D insufficiency in TgAb-positive subjects was significantly higher than that observed in TPOAb and TgAb-negative subjects, whether based on cutoff values of 20 or 30 ng/mL: 8.3% vs 5.6%, p < 0.05; or 47.6% vs 42.0%, p < 0.05, respectively. However, vitamin D status was not associated with positive TPOAb and/or TgAb after controlling for gender and age. To explore the probable interaction between vitamin D status and age on serum TSH, analyses were performed according to age tertiles, it was found that higher 25(OH)D levels were independently associated with lower TSH, but only in subjects in the lowest age tertile.
Conclusions: This population-based study showed that high vitamin D status in younger individuals is associated with low circulating thyrotropin.
TSH wikipedia
has the following graphic
237 items in PubMed title: thyroid OR hyperthyroid AND vitamin d the title
The Role of Vitamin D in Autoimmune Thyroid Diseases: A Narrative Review - Feb 2023
Vitamin D and the Thyroid: A Critical Review of the Current Evidence - Feb 2023
RCT Quality for Vitamin D and Thyroid - 2022
Assessment of the reporting quality of randomised controlled trials for vitamin D supplementation in autoimmune thyroid disorders based on the CONSORT statement
Vitamin D-Related Genes and Thyroid Cancer-A Systematic Review - Nov 2022
Association Between Vitamin D Deficiency and Autoimmune Thyroid Disorder: A Systematic Review - June 2022
Association of Vitamin D Pathway Genetic Variation and Thyroid Cancer. July 2019 Free PDF
The Role of Vitamin D in Thyroid Diseases.= July 2018 FREE PDF
Vitamin D and thyroid diseases. 2016] Free PDF
Vitamin D in thyroid disorders July 2015
Fix Thyroid then increase vitamin D - Oct 2013
Fix Thyroid then increase vitamin D - Oct 2013
Includes PDF. PPT, and audio of the presentation
Brief summary
If you have any Thyroid problems, do not take Vitamin D until you have corrected other problems like Adrenal Deficiency
Start with 1,000 IU vitamin D daily for the first week
Increase by 1,000 IU each week for 3+ weeks
Should also increase Iodine
Thyroid Supplements With a Kick New York Times, Jan 2014
Nothing about vitamin D, but interesting
Researchers who tested 10 popular thyroid-boosting products sold online found that nine contained the hormones
- thyroxine (T4) or triiodothyronine (T3), sometimes both.
- one supplement delivered 91 micrograms of T4 and 16.5 micrograms of T3 (more than in some prescription drugs)
While looking at the above journal article I did a query for Vitamin D and found the following - Jan 2014
Low Levels of Serum Vitamin D3 are Associated with Autoimmune Thyroid Disease in Pre-Menopausal Women Thyroid Journal, Dec 2013
Background: Low serum vitamin D level has been associated with several autoimmune diseases, but its association with thyroid autoimmunity is unclear.
We evaluated the association of serum vitamin D level with the prevalence of autoimmune thyroid disease (AITD).
Methods: Our cross-sectional study included subjects who underwent routine health check-ups, which included assays of serum 25-hydroxy vitamin D3 (25(OH)D3) and anti-thyroid peroxidase antibody (TPO-Ab), as well as thyroid ultrasonography (US) between 2008 and 2012 at Asan Medical Center. We defined AITD according to the level of TPO-Ab and US findings.
Results: Total 6,685 subjects (Male, 58%; Female, 42%) were enrolled for this study. Overall prevalence of TPO-Ab positivity and both TPO-Ab/US positivity were 10.1% (Male, 6.3%; Female, 15.3%) and 5.4% (Male, 2.3%; Female, 9.7%), respectively. In female subjects, mean serum 25(OH)D3 levels were significantly lower in TPO-Ab(+) ( 22.0 vs. 23.5 ng/mL , P=0.030), and TPO-Ab(+)/US(+) group (21.6 vs. 23.4 ng/mL, P=0.027) as compared with corresponding control group, respectively. According to the level of serum 25(OH)D3, the prevalence of TPO-Ab positivity (21.2%, 15.5% and 12.6% in deficient, insufficient, and sufficient group, respectively, P=0.001) and both TPO-Ab/US positivity (14.7%, 9.9% and 7.1% in deficient, insufficient, and sufficient group, respectively, P<0.001) was decreased in female subjects. Interestingly, this pattern was significant only in pre-menopausal women (P=0.003 and P<0.001, respectively), but not in post-menopausal women. Multivariate analysis indicated that the adjusted odds ratios (OR) for AITD among those in the 25(OH)D3-deficient (TPO-Ab(+); OR=1.95, P=0.001 and TPO-Ab(+)/US(+); OR=2.36, P<0.001), and -insufficient group (TPO-Ab(+); OR=1.31, P=0.043 and TPO-Ab(+)/US(+); OR=1.50, P=0.017) were significantly increased when compared with -sufficient group.
Conclusions: The level of serum vitamin D was significantly lower in pre-menopausal women with AITD.
Vitamin D deficiency and insufficiency were significantly associated with AITD in pre-menopausal women.
Note - that is not much of a difference in Vitamin D levels.
2800 IU vitamin D helped when given both before and after parathyroidectomy - March 2014
Vitamin D treatment in primary hyperparathyroidism: a randomized placebo controlled trial.
J Clin Endocrinol Metab. 2014 Mar;99(3):1072-80. doi: 10.1210/jc.2013-3978. Epub 2014 Jan 13.
Rolighed L1, Rejnmark L, Sikjaer T, Heickendorff L, Vestergaard P, Mosekilde L, Christiansen P.
CONTEXT:
Low 25-hydroxyvitamin D levels are common in patients with primary hyperparathyroidism (PHPT) and associated with higher PTH levels and hungry bone syndrome after parathyroidectomy (PTX). However, concerns have been raised about the safety of vitamin D supplementation in PHPT.
OBJECTIVE:
We aimed to assess safety and effects on calcium homeostasis and bone metabolism of supplementation with high doses of vitamin D in PHPT patients.
DESIGN, SETTING:
This was an investigator-initiated double-blind, randomized, placebo-controlled, parallel-group trial from a single center.
PATIENTS:
Forty-six PHPT patients were recruited, with a mean age of 58 (range 29-77) years, and 35 (76%) were women.
INTERVENTIONS:
Intervention included daily supplementation with 70 μg (2800 IU) cholecalciferol or identical placebo for 52 weeks. Treatment was administered 26 weeks before PTX and continued for 26 weeks after PTX.
MAIN OUTCOME MEASURES:
PTH, calcium homeostasis, and bone metabolism were evaluated.
RESULTS:
Preoperatively, 25-hydroxyvitamin D increased from 50 to 94 nmol/L in the treatment group and decreased from 57 to 52 nmol/L in the placebo group (P < .001). Compared with placebo, vitamin D decreased PTH significantly by 17% before PTX (P = .01), increased lumbar spine bone mineral density by 2.5% (P = .01), and decreased C-terminal β-CrossLaps by 22% (P < .005). The trabecular bone score did not change in response to treatment, but improved after PTX. Postoperatively, PTH remained lower in the cholecalciferol group compared with the placebo group (P = .04). Plasma creatinine and plasma and urinary calcium did not differ between groups.
CONCLUSIONS:
Daily supplementation with a high vitamin D dose safely improves vitamin D status and decreases PTH in PHPT patients. The vitamin D treatment is accompanied by reduced bone resorption and improved bone mineral density before operation.