Omega-3 – need more than 1 gram for a short time to reduce Cardiovascular Disease
Omega-3 Fatty Acids and Cardiovascular Disease: Are There Benefits?
Current Treatment Options in Cardiovascular Medicine, November 2016, 18:69; DOI: 10.1007/s11936-016-0487-1
Kate J. BowenWilliam S. HarrisPenny M. Kris-Etherton
 Items in both categories Omega-3 Cardiovascular are listed here:
{category}
Pages listed in BOTH the categories Magnesium and Cardiovascular
{category}
Items in both categories Omega-3 Cardiovascular are listed here:
{category}
Pages listed in BOTH the categories Magnesium and Cardiovascular
{category}
📄 Download the PDF from VitaminDWiki
Opinion statement
Early secondary prevention trials of fish and omega-3 polyunsaturated fatty acid (PUFA) capsules reported beneficial effects on cardiovascular disease (CVD) outcomes, including all-cause mortality and sudden cardiac death. These clinical findings, as well as observational and experimental data, demonstrated that omega-3 PUFAs reduced the risk of coronary outcomes and overall mortality and were the basis for recommendations made in the early 2000s to increase omega-3 PUFA intake. In the last 6 years, however, results from both primary and secondary prevention trials have generally failed to show a beneficial effect of omega-3 PUFA supplementation, bringing current recommendations into question.
Several possible reasons for these null findings have been proposed,
including short treatment periods,
relatively low doses of omega-3 PUFAs,
small sample sizes,
higher background omega-3 intakes, and the
concurrent use of modern pharmacotherapy for CVD prevention.
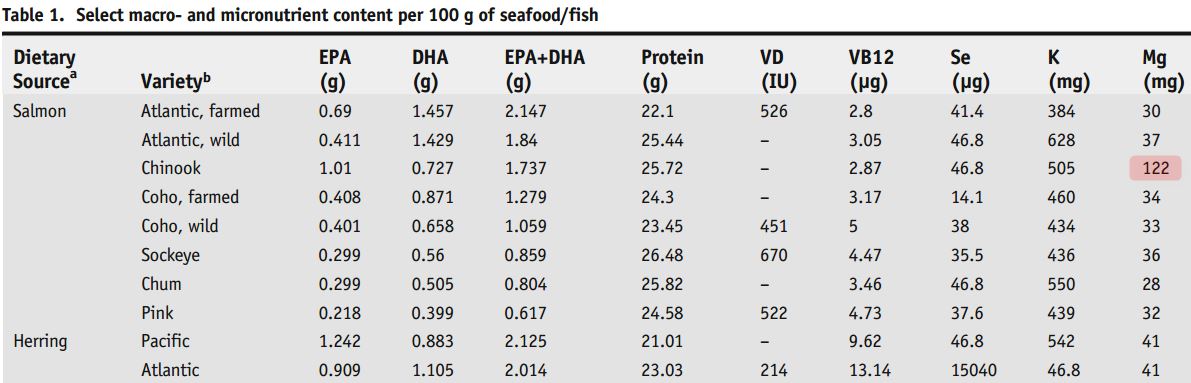
At least one of these caveats is being assessed in major clinical trials, with two omega-3 PUFA pharmacological agents being tested at doses of 4?g/day (instead of the more common <1 g/day). These null findings, however, do not necessarily mean that omega-3 PUFAs “are ineffective” in general, only that they were not effective in the context in which they were tested. Accordingly, higher intakes of omega-3 PUFAs, either from fatty fish or from supplements, if continued for decades (as the epidemiological data support) are likely to contribute towards lower risk for CVD. At this time, evidence supports the consumption of a healthy dietary pattern with at least two servings per week of fatty fish. Omega-3 PUFA supplementation is a reasonable alternative for those who do not consume fish, although fish is the preferred source of omega-3 PUFAs because it also provides additional nutrients, some of which are often under-consumed.