Multiple Sclerosis 40% more likely in obese than in overweight (Mendelian randomization)
Mendelian randomization in multiple sclerosis: A causal role for vitamin D and obesity?
Multiple Sclerosis Journal, January 8, 2018
Adil Harroud, J Brent Richards
📄 Download the PDF from VitaminDWiki
The etiology of multiple sclerosis (MS) involves a complex interplay of genetic and environmental factors. Epidemiologic studies have furthered our understanding of these risk factors but remain limited by residual confounding and potential for reverse causation, particularly in MS where time of disease onset is not known. Mendelian randomization (MR) uses genetic variants to study the causal effect of modifiable exposures on an outcome. This method avoids some of the limitations of classical epidemiology and can strengthen causal inference. Here, we introduce the basic concepts of MR and review its contributions to the field of MS. Indeed, several studies using MR have now provided support for a causal role for low vitamin D level and obesity in the development of MS.
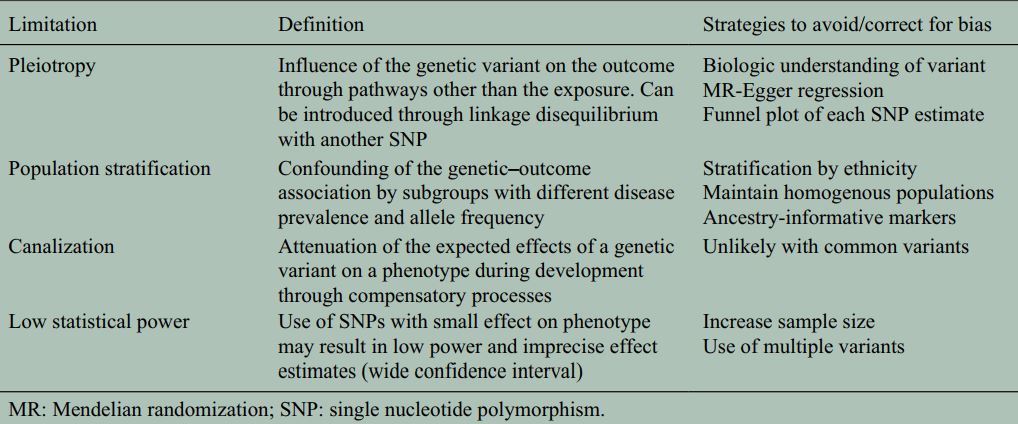
Table 1. Limitations of MR and how to address them
References
1. Olsson, T, Barcellos, LF, Alfredsson, L. Interactions between genetic, lifestyle and environmental risk factors for multiple sclerosis. Nat Rev Neurol 2017; 13: 25–36. Google Scholar, Crossref, Medline
2. Van der Mei, I, Lucas, RM, Taylor, BV. Population attributable fractions and joint effects of key risk factors for multiple sclerosis. Mult Scler 2016; 22: 461–469. Google Scholar, Link
3. International Multiple Sclerosis Genetics Consortium, Beecham, AH, Patsopoulos, NA. Analysis of immune-related loci identifies 48 new susceptibility variants for multiple sclerosis. Nat Genet 2013; 45: 1353–1360. Google Scholar, Crossref, Medline
4. Smith, GD, Lawlor, DA, Harbord, R. Clustered environments and randomized genes: A fundamental distinction between conventional and genetic epidemiology. PLoS Med 2007; 4: e352. Google Scholar, Crossref, Medline
5. Marrie, RA, Yu, N, Wei, Y. High rates of physician services utilization at least five years before multiple sclerosis diagnosis. Mult Scler 2013; 19: 1113–1119. Google Scholar, Link
6. Hughes, AM, Lucas, RM, McMichael, AJ. Early-life hygiene-related factors affect risk of central nervous system demyelination and asthma differentially. Clin Exp Immunol 2013; 172: 466–474. Google Scholar, Crossref, Medline
7. Magyari, M, Koch-Henriksen, N, Pfleger, CC. Reproduction and the risk of multiple sclerosis. Mult Scler 2013; 19: 1604–1609. Google Scholar, Link
8. Hedstrom, AK, Hillert, J, Olsson, T. Reverse causality behind the association between reproductive history and MS. Mult Scler 2014; 20: 406–411. Google Scholar, Link
9. Lawlor, DA, Harbord, RM, Sterne, JA. Mendelian randomization : Using genes as instruments for making causal inferences in epidemiology. Stat Med 2008; 27: 1133–1163. Google Scholar, Crossref, Medline
10. Mokry, LE, Ahmad, O, Forgetta, V. Mendelian randomisation applied to drug development in cardiovascular disease: A review. J Med Genet 2015; 52: 71–79. Google Scholar, Crossref, Medline
11. Nielsen, NM, Munger, KL, Koch-Henriksen, N. Neonatal vitamin D status and risk of multiple sclerosis: A population-based case-control study. Neurology 2017; 88: 44–51. Google Scholar, Crossref, Medline
12. Davey Smith, G, Hemani, G. Mendelian randomization : Genetic anchors for causal inference in epidemiological studies. Hum Mol Genet 2014; 23: R89–98. Google Scholar, Crossref, Medline
13. Bowden, J, Davey Smith, G, Burgess, S. Mendelian randomization with invalid instruments: Effect estimation and bias detection through Egger regression. Int J Epidemiol 2015; 44: 512–525. Google Scholar, Crossref, Medline
14. Interleukin-6 Receptor Mendelian Randomisation Analysis Consortium, Swerdlow, DI, Holmes, MV. The interleukin-6 receptor as a target for prevention of coronary heart disease: A Mendelian randomisation analysis. Lancet 2012; 379: 1214–1224. Google Scholar, Crossref, Medline
15. Kleveland, O, Kunszt, G, Bratlie, M. Effect of a single dose of the interleukin-6 receptor antagonist tocilizumab on inflammation and troponin T release in patients with non-ST-elevation myocardial infarction: A double-blind, randomized, placebo-controlled phase 2 trial. Eur Heart J 2016; 37: 2406–2413. Google Scholar, Crossref, Medline
16. Burgess, S, Timpson, NJ, Ebrahim, S. Mendelian randomization : Where are we now and where are we going? Int J Epidemiol 2015; 44: 379–388. Google Scholar, Crossref, Medline
17. Noyce, AJ, Nalls, MA. Mendelian randomization –The key to understanding aspects of Parkinson’s disease causation? Mov Disord 2016; 31: 478–483. Google Scholar, Crossref, Medline
18. Looker, AC, Pfeiffer, CM, Lacher, DA. Serum 25-hydroxyvitamin D status of the US population: 1988–1994 compared with 2000–2004. Am J Clin Nutr 2008; 88: 1519–1527. Google Scholar, Crossref, Medline
19. Flegal, KM, Kruszon-Moran, D, Carroll, MD. Trends in obesity among adults in the United States, 2005 to 2014. JAMA 2016; 315: 2284–2291. Google Scholar, Crossref, Medline
20. Salzer, J, Hallmans, G, Nystrom, M. Vitamin D as a protective factor in multiple sclerosis. Neurology 2012; 79: 2140–2145. Google Scholar, Crossref, Medline
21. Munger, KL, Levin, LI, Hollis, BW. Serum 25-hydroxyvitamin D levels and risk of multiple sclerosis. JAMA 2006; 296: 2832–2838. Google Scholar, Crossref, Medline
22. Munger, KL, Zhang, SM, O’Reilly, E. Vitamin D intake and incidence of multiple sclerosis. Neurology 2004; 62: 60–65. Google Scholar, Crossref, Medline
23. Mokry, LE, Ross, S, Ahmad, OS. Vitamin D and risk of multiple sclerosis: A Mendelian randomization Study. PLoS Med 2015; 12: e1001866. Google Scholar, Crossref, Medline
24. International Multiple Sclerosis Genetics Consortium, Wellcome Trust Case Control Consortium, Sawcer, S. Genetic risk and a primary role for cell-mediated immune mechanisms in multiple sclerosis. Nature 2011; 476: 214–219. Google Scholar, Crossref, Medline
25. Rhead, B, Baarnhielm, M, Gianfrancesco, M. Mendelian randomization shows a causal effect of low vitamin D on multiple sclerosis risk. Neurol Genet 2016; 2: e97. Google Scholar, Crossref, Medline
26. Gianfrancesco, MA, Stridh, P, Rhead, B. Evidence for a causal relationship between low vitamin D, high BMI, and pediatric-onset MS . Neurology 2017; 88: 1623–1629. Google Scholar, Crossref, Medline
27. Munger, KL, Chitnis, T, Ascherio, A. Body size and risk of MS in two cohorts of US women. Neurology 2009; 73: 1543–1550. Google Scholar, Crossref, Medline
28. Langer-Gould, A, Brara, SM, Beaber, BE. Childhood obesity and risk of pediatric multiple sclerosis and clinically isolated syndrome. Neurology 2013; 80: 548–552. Google Scholar, Crossref, Medline
29. Munger, KL, Bentzen, J, Laursen, B. Childhood body mass index and multiple sclerosis risk: A long-term cohort study. Mult Scler 2013; 19: 1323–1329. Google Scholar, Link
30. Hedstrom, AK, Olsson, T, Alfredsson, L. Body mass index during adolescence, rather than childhood, is critical in determining MS risk. Mult Scler 2016; 22: 878–883. Google Scholar, Link
31. Mokry, LE, Ross, S, Timpson, NJ. Obesity and multiple sclerosis: A Mendelian randomization study. PLoS Med 2016; 13: e1002053. Google Scholar, Crossref, Medline
32. Locke, AE, Kahali, B, Berndt, SI. Genetic studies of body mass index yield new insights for obesity biology. Nature 2015; 518: 197–206. Google Scholar, Crossref, Medline
33. Gianfrancesco, MA, Glymour, MM, Walter, S. Causal effect of genetic variants associated with Body Mass Index on multiple sclerosis susceptibility. Am J Epidemiol 2017; 185: 162–171. Google Scholar, Medline
34. Felix, JF, Bradfield, JP, Monnereau, C. Genome-wide association analysis identifies three new susceptibility loci for childhood Body Mass Index. Hum Mol Genet 2016; 25: 389–403. Google Scholar, Crossref, Medline
35. Pierce, BL, Ahsan, H, Vanderweele, TJ. Power and instrument strength requirements for Mendelian randomization studies using multiple genetic variants. Int J Epidemiol 2011; 40: 740–752. Google Scholar, Crossref, Medline
36. Sovio, U, Mook-Kanamori, DO, Warrington, NM. Association between common variation at the FTO locus and changes in body mass index from infancy to late childhood: The complex nature of genetic association through growth and development. PLoS Genet 2011; 7: e1001307. Google Scholar, Crossref, Medline
37. Pakpoor, J, Pakpoor, J. Childhood obesity and risk of pediatric multiple sclerosis and clinically isolated syndrome. Neurology 2013; 81: 1366. Google Scholar, Crossref, Medline
38. Vimaleswaran, KS, Berry, DJ, Lu, C. Causal relationship between obesity and vitamin D status: Bi-directional Mendelian randomization analysis of multiple cohorts. PLoS Med 2013; 10: e1001383. Google Scholar, Crossref, Medline
39. Kraszula, L, Jasinska, A, Eusebio, M. Evaluation of the relationship between leptin, resistin, adiponectin and natural regulatory T cells in relapsing-remitting multiple sclerosis. Neurol Neurochir Pol 2012; 46: 22–28. Google Scholar, Crossref, Medline
40. Piccio, L, Cantoni, C, Henderson, JG. Lack of adiponectin leads to increased lymphocyte activation and increased disease severity in a mouse model of multiple sclerosis. Eur J Immunol 2013; 43: 2089–2100. Google Scholar, Crossref, Medline
41. Devorak, J, Mokry, LE, Morris, JA. Large differences in adiponectin levels have no clear effect on multiple sclerosis risk: A Mendelian randomization study. Mult Scler 2016: 1352458516681196. Google Scholar
42. Hedstrom, AK, Lima Bomfim, I, Barcellos, L. Interaction between adolescent obesity and HLA risk genes in the etiology of multiple sclerosis. Neurology 2014; 82: 865–872. Google Scholar, Crossref, Medline