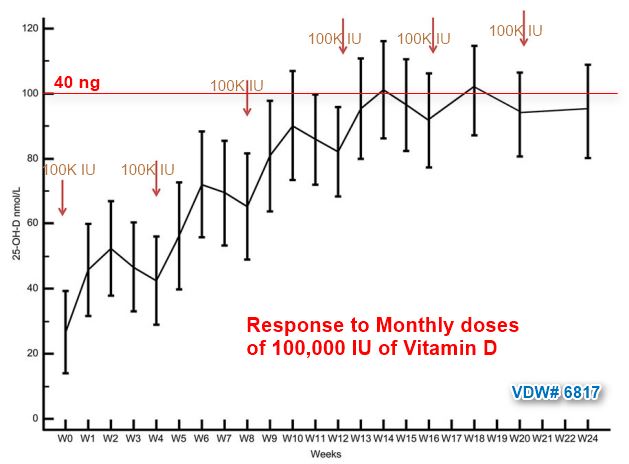
Monthly 100,000 IU of Vitamin D adds about 25 ng - RCT
What Factors Modify the Effect of Monthly Bolus Dose Vitamin D Supplementation on 25-hydroxyvitamin D Concentrations?
J Steroid Biochem Mol Biol. 2020 Jul;201:105687. doi: 10.1016/j.jsbmb.2020.105687
Zhenqiang Wu 1, Carlos A Camargo Jr 2, Ian R Reid 3, Angela Beros 1, John D Sluyter 1, Debbie Waayer 1, Carlene M M Lawes 1, Les Toop 4, Kay-Tee Khaw 5, Robert Scragg 6
 * Monthly 100,000 IU vitamin D supplementation got virtually all vitamin D deficient subjects above 20 ng – RCT April 2014
* Monthly 100,000 IU of vitamin D is safe (and may be better than daily) – RCT Aug 2018
* One pill every two weeks gives you all the vitamin D most adults need
* RCTs for 22 health problems with 50,000 IU / 2 weeks - should be slightly better than 100,000 IU / 4 weeks
* Less bone loss if take 100,000 IU vitamin D monthly – RCT Nov 2017
* 100,000 IU of Vitamin D3 monthly for 4 months to diabetics (D2 bombed) – RCT Dec 2019
*
* Monthly 100,000 IU vitamin D supplementation got virtually all vitamin D deficient subjects above 20 ng – RCT April 2014
* Monthly 100,000 IU of vitamin D is safe (and may be better than daily) – RCT Aug 2018
* One pill every two weeks gives you all the vitamin D most adults need
* RCTs for 22 health problems with 50,000 IU / 2 weeks - should be slightly better than 100,000 IU / 4 weeks
* Less bone loss if take 100,000 IU vitamin D monthly – RCT Nov 2017
* 100,000 IU of Vitamin D3 monthly for 4 months to diabetics (D2 bombed) – RCT Dec 2019
* 
📄 Download the PDF from sci-hub via VitaminDWiki
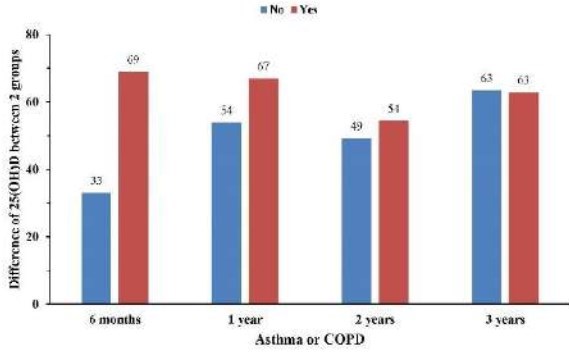
Some unexpected results (All charts show increases vs those taking placebo in nmol)
2X bigger increase initially if have COPD or Asthma, little difference at 3 years
Response similar by normal and overweight at 1 and 2 years

More hours of sun resulted in less response to monthly supplement

The increasing use of vitamin D supplements has stimulated interest in identifying factors that may modify the effect of supplementation on circulating 25-hydroxyvitamin D (25(OH)D) concentrations. Such information is of potential interest to researchers, clinicians and patients when deciding on bolus dose of vitamin D supplementation.
We carried out a large randomized controlled trial of 5110 adults aged 50-84 years, of European/Other (84%), Polynesian (11%) and Asian (5%) ethnicity, to whom we gave a standard dose of vitamin D3 supplements (200,000 IU initially, then 100,000 IU monthly) which was taken with high adherence.
All participants provided a baseline blood sample, and follow-up blood samples were collected at 6 months and annually for 3 years in a random sample of 441 participants, and also at 2 years in 413 participants enrolled in a bone density sub-study. Serum 25(OH)D was measured by LC/MSMS. Mixed model analyses were carried out on all 854 participants providing follow-up blood samples in multivariable models that included age, sex, ethnicity, body mass index (kg/m2), tobacco smoking, alcohol intake, physical activity, sun exposure, season, medical prescription of high-dose vitamin D3 (Cal.D.Forte tablets), asthma/COPD and the study treatment (vitamin D or placebo).
The adjusted mean difference in 25(OH)D in the follow-up points between vitamin D supplementation and placebo groups was inversely related (all p for interaction <0.05) to baseline 25(OH)D, BMI, and hours of sun exposure, and higher in females, elders, and those with high frequency of alcohol, medical prescription of vitamin D, and asthma/COPD. The mean difference was not significantly related to ethnicity (p = 0.12), tobacco (p = 0.34), and vigorous activity (p = 0.33).
In summary, these data show that vitamin D status, BMI, sun exposure hours, sex and asthma/COPD modify the 25(OH)D response to vitamin D supplementation. By contrast, ethnicity, tobacco smoking, and vigorous activity do not.