Higher Omega-3 index (4 to 8 percent) associated with 30 percent less risk of coronary disease (10 studies)
The Omega-3 Index and relative risk for coronary heart disease mortality: Estimation from 10 cohort studies
Atherosclerosis, July 2017 Volume 262, Pages 51–54
DOI: http://dx.doi.org/10.1016/j.atherosclerosis.2017.05.007
William S. Harris', William S. Harris, William S. Harris, Liana Del Gobbo, Nathan L. Tintle
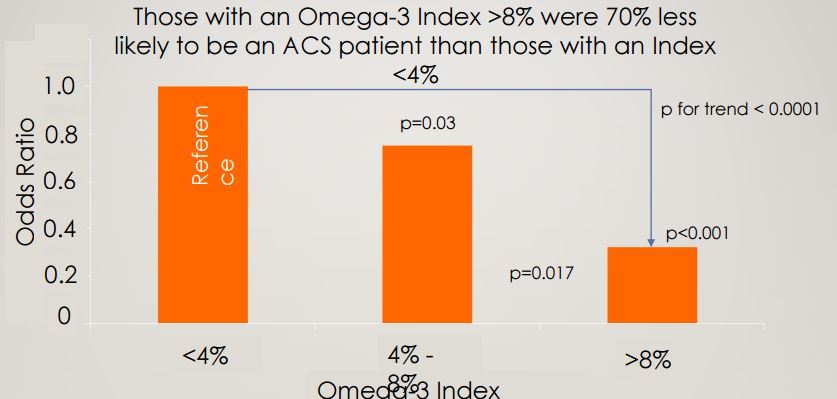
 * Acute Coronary Syndrome risk reduced with higher levels of Omega-3
*
* Acute Coronary Syndrome risk reduced with higher levels of Omega-3
*  ---
Omega-3 index = % of the total amount of fatty acids present in red blood cell
* Thus, the higher the index, the lower must be the Omega-6 %
* So, to improve the Omega-3 index, one must both increase Omega-3 intake and decrease intake of other fatty acids, such as Omega-6
1. Omega-3 and Cardiovascular (items in both categories)
{category}
---
Omega-3 index = % of the total amount of fatty acids present in red blood cell
* Thus, the higher the index, the lower must be the Omega-6 %
* So, to improve the Omega-3 index, one must both increase Omega-3 intake and decrease intake of other fatty acids, such as Omega-6
1. Omega-3 and Cardiovascular (items in both categories)
{category}
📄 Download the PDF from VitaminDWiki
Highlights
•Higher in vivo omega-3 levels are linked with lower risk for heart disease.
•Omega-3 status is currently expressed using several different metrics.
•The Omega-3 Index (O3I, RBC EPA + DHA) is a useful marker but cutpoints need validation.
•Transformed data from a prior meta-analysis confirms O3I cutpoints of <4% and >8%.
Background and aims
A recent 19-cohort meta-analysis examined the relationships between biomarkers of omega-3 fatty acids and risk for coronary heart disease (CHD). That study did not, however, report hazard ratios (HRs) specifically as a function of erythrocyte eicosapentaenoic (EPA) plus docosahexaenoic (DHA) levels, a metric called the Omega-3 Index in which EPA + DHA content is expressed as a percent of total fatty acids. The Omega-3 Index has been used in several recent studies and is a validated biomarker of omega-3 fatty acid tissue levels, but additional data are needed to confirm (or refute) the originally-proposed clinical cut-points of <4% (higher risk) and 8%–12% (lower risk).
Methods
The present study was therefore undertaken using published data from this meta-analysis to estimate HRs per 1-SD increase in the Omega-3 Index and median quintile values for this metric across 10 of the cohorts for which the needed data were available.
Results
The overall mean (SD) for the Omega-3 Index in these 10 cohort studies was 6.1% (2.1%), and the HR for a 1-SD increase was 0.85 (95% confidence interval, 0.80–0.91). Median quintile 1 and 5 levels were 4.2% vs. 8.3%, respectively. Based on these values, we estimate that risk for fatal CHD would have been reduced by about 30% moving from an Omega-3 Index of 4%–8%.
Conclusions
These findings support the use of <4% and >8% as reasonable therapeutic targets for the Omega-3 Index