3.3 X more likely to die if infected with SARS-Cov-2 plus a second pathogen – meta-analysis
Prevalence and outcomes of co-infection and superinfection with SARS-CoV-2 and other pathogens: A systematic review and meta-analysis
PLOS X https://doi.org/10.1371/journal.pone.0251170
Jackson S. Musuuza, Lauren Watson, Vishala Parmasad, Nathan Putman-Buehler, Leslie Christensen, Nasia Safdar
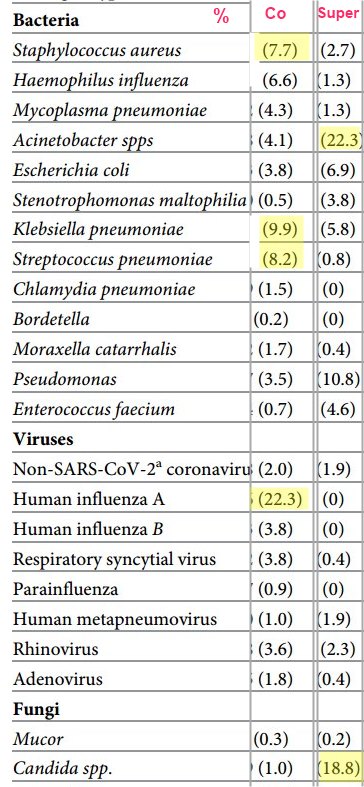
Note Many of the pathogens are associated with low vitamin D:
Examples: acinetobacter, human influenza A, Aklebsiella pneumoniae
Introduction
The recovery of other pathogens in patients with SARS-CoV-2 infection has been reported, either
at the time of a SARS-CoV-2 infection diagnosis (co-infection) or
subsequently (superinfection) .
However, data on the prevalence, microbiology, and outcomes of co-infection and superinfection are limited. The purpose of this study was to examine the occurrence of co-infections and superinfections and their outcomes among patients with SARS-CoV-2 infection.
Patients and methods
We searched literature databases for studies published from October 1, 2019, through February 8, 2021. We included studies that reported clinical features and outcomes of co-infection or superinfection of SARS-CoV-2 and other pathogens in hospitalized and non-hospitalized patients. We followed PRISMA guidelines, and we registered the protocol with PROSPERO as: CRD42020189763.
Results
Of 6639 articles screened, 118 were included in the random effects meta-analysis. The pooled prevalence of
co-infection was 19% (95% confidence interval [CI]: 14%-25%, I2 = 98%) and that of
superinfection was 24% (95% CI: 19%-30%).
Pooled prevalence of pathogen type stratified by co- or superinfection were:
viral co-infections, 10% (95% CI: 6%-14%);
- viral superinfections, 4% (95% CI: 0%-10%);
bacterial co-infections, 8% (95% CI: 5%-11%);
- bacterial superinfections, 20% (95% CI: 13%-28%);
fungal co-infections, 4% (95% CI: 2%-7%); and
- fungal superinfections, 8% (95% CI: 4%-13%).
Patients with a co-infection or superinfection had higher odds of dying than those who only had SARS-CoV-2 infection (odds ratio = 3.31 , 95% CI: 1.82–5.99). Compared to those with co-infections, patients with superinfections had a higher prevalence of mechanical ventilation (45% [95% CI: 33%-58%] vs. 10% [95% CI: 5%-16%]), but patients with co-infections had a greater average length of hospital stay than those with superinfections (mean = 29.0 days, standard deviation [SD] = 6.7 vs. mean = 16 days, SD = 6.2, respectively).
Conclusions
Our study showed that as many as 19% of patients with COVID-19 have co-infections and 24% have superinfections. The presence of either co-infection or superinfection was associated with poor outcomes, including increased mortality. Our findings support the need for diagnostic testing to identify and treat co-occurring respiratory infections among patients with SARS-CoV-2 infection.